

To analyze postoperative infections in critically ill patients undergoing heart surgery.
SettingIntensive care units (ICUs).
DesignAn observational, prospective, multicenter study was carried out.
PatientsPatients in the postoperative period of heart surgery admitted to the ICU and included in the ENVIN-HELICS registry between 2005 and 2011.
Main outcome variablesMechanical ventilation associated pneumonia (MVP), urinary catheter-related infection (UCI), primary bacteremia (PB), PB related to vascular catheters (PB-VC) and secondary bacteremia.
ResultsOf a total of 97,692 patients included in the study, 9089 (9.3%) had undergone heart surgery. In 440 patients (4.8%), one or more infections were recorded. Infection rates were 9.94 episodes of MVP per 1000 days of mechanical ventilation, 3.4 episodes of UCI per 1000 days of urinary catheterization, 3.10 episodes of BP-VC per 1000 days of central venous catheter, and 1.84 episodes of secondary bacteremia per 1000 days of ICU stay. Statistically significant risk factors for infection were ICU stay (odds ratio [OR] 1.18, 95%CI 1.16–1.20), APACHE II upon admission to the ICU (OR 1.05, 95%CI 1.03–1.07), emergency surgery (OR 1.67, 95%CI 1.13–2.47), previous antibiotic treatment (OR 1.38, 95%CI 1.04–1.83), and previous colonization by Pseudomonas aeruginosa (OR 18.25, 95%CI 3.74–89.06) or extended spectrum beta-lactamase producing enterobacteria (OR 16.97, 95%CI 5.4–53.2). The overall ICU mortality rate was 4.1% (32.2% in patients who developed one or more infections and 2.9% in uninfected patients) (p<.001).
ConclusionsOf the patients included in the ENVIN-HELICS registry, 9.3% were postoperative heart surgery patients. The overall mortality was low but increased significantly in patients who developed one or more infection episodes.
Analizar las infecciones en Pacientes críticos postOperados de Cirugía Cardiaca (POCC).
ÁmbitoUnidades de cuidados intensivos (UCI).
DiseñoEstudio observacional, prospectivo y multicéntrico.
PacientesSe incluyeron los pacientes POCC incluidos en el registro ENVIN-HELICS entre los años 2005-2011.
Variables de interés principalNeumonías relacionadas con ventilación mecánica (N-VM), infecciones urinarias relacionadas con sonda uretral (IU-SU), bacteriemias primarias y/o relacionadas con catéteres vasculares (BP-BCV) y bacteriemias secundarias (BS).
ResultadosDe los 97.692 pacientes registrados 9.089 (9,3%) fueron POCC. En 440 (4,8%) POCC se identificaron una o más de las infecciones controladas. La densidad de infección fue de 9,94 episodios de N-VM por 1.000 días de VM; 3,4 episodios de IU-SU por 1.000 días de SU, 3,10 episodios de BP-BCV por 1.000 días de CVC; y 1,84 episodios de BS por 1.000 días de estancia en UCI. Los factores de riesgo estadísticamente significativos fueron estancia en UCI (OR 1,18; IC95% 1,16-1,20), APACHE II al ingreso en UCI (OR 1,05; IC95% 1,03-1,07), cirugía urgente (OR 1,67; IC95% 1,13-2,47), tratamiento antibiótico previo (OR 1,38; IC95% 1,04-1,83), colonización previa de Pseudomonas aeruginosa (OR 18,25; IC95% 3,74-89,06) o enterobacterias productoras de betalactamasas de espectro extendido (OR 16,97; IC95% 5,4-53,2). La mortalidad intra-UCI fue del 4,1%; del 32,2% en aquellos que desarrollaron una o más infecciones y del 2,9% en los pacientes sin infección (p<0,001).
ConclusionesEl 9,3% de los pacientes incluidos en el registro fueron POCC. La mortalidad global de los POCC es baja pero aumenta significativamente en aquellos que desarrollaron una o más infecciones.
The number of patients needing heart surgery has increased in recent years. The postoperative period of this kind of surgery initially requires the adoption of a series of therapeutic and/or monitorization measures for which the patient must stay in specialized units such as the Department of Intensive Care Medicine or the Intensive Care Unit (ICU) for a number of days after the operation. In the great majority of cases the patient course is favorable, though a small group of individuals can suffer a range of complications. One of the possible complications in the immediate postoperative period is the development of infections associated to invasive devices (tracheal tube, ventilator, urethral catheter, vascular catheters) used during surgery and in the subsequent days. The presence of these infections has been related to an increase in morbidity and mortality.1
In Spain, the monitoring of infections acquired in the ICU is fundamentally carried out by means of the ENVIN-HELICS registry, developed by the Infectious Diseases Working Group of the Spanish Society of Intensive and Critical Care Medicine and Coronary Units (SEMICYUC).2 For years, this registry has established a longitudinal control of patients admitted to the ICU for more than 24h, with the purpose of identifying infections related to invasive devices, and to know the consumption of antimicrobials during admission to the ICU. One of its options is patient classification according to background disease, with a specific code for postoperative heart surgery patients (POHS). In this study we describe the device-related infection rates, characteristics and etiologies in POHS, along with the risk factors for these infections in this particular subgroup of patients.
Materials and methodsPatients studiedWe selected the patients included in the ENVIN-HELICS registry between the years 2005 and 2011 (both included), with a main diagnosis of “postoperative period of heart surgery” (identified by code 113). This registry contemplates voluntary participation on the part of the different ICUs, with free access (using a code for each ICU) on the Internet: http://hws.vhebron.net/envin-helics/. The registry includes all the patients admitted for more than 24h to the participating ICUs during the months from April to June of each year. The information is directly entered in a centralized database with an analytical program allowing each participating ICU to know its own results and also the global national results. The national report corresponding to each year is distributed among all Spanish hospitals and can be accessed from the SEMICYUC website: http://www.semicyuc.org/.3
Monitoring methodologyThe patients admitted before the first day of the control period and who remained admitted during the study phase were not subjected to follow-up. Monitoring of the patients included in the study was continuous, with follow-up until discharge from the ICU or for a maximum of 30 days.
The following data were collected for all included patients: demographic variables, background disease, instrumentation performed (intubation and mechanical ventilation [MV], urethral catheterization, central venous and arterial catheterization), hospital stay prior to admission to the ICU, stay in the ICU, and clinical condition at the time of discharge. The severity of the patients was evaluated by the combination of the APACHE II score4 and, optionally, using the SAPS II system5 in the first 24h of admission to the ICU, and the need for urgent surgery, defined as non-elective surgery before or during ICU stay. Raw mortality was defined as fatalities due to any reason, occurring during the stay in the ICU.
Infections studiedAn analysis has been made of the infections directly associated with the use of invasive devices, such as ventilator associated pneumonia (VAP), urethral catheter related urinary infection (UCI), primary bacteremia (PB) and PB related to vascular catheters (PB-VC), and bacteremia acquired in the ICU secondary to other foci (SB). The vascular catheters considered to pose a risk in this study were central venous catheters and arterial catheters. The criteria used to define these infections have been published in the manual of the ENVIN project,2 following the indications of the CDC.6 We did not register surgical wound related superficial or deep infections, except when of a bacteremic nature.
The infections related to invasive devices were diagnosed by the physicians in charge of patient care, and were documented as such in the case history. The physicians in charge of monitoring nosocomial infections were specialists in intensive care medicine with a special interest and training in infectious diseases. These physicians prospectively registered the infections but did not intervene directly in their diagnosis.
For the etiological diagnosis we accepted the criteria used by each participating ICU. Susceptibility to the different antibiotics of the pathogens identified as being responsible for the infection was established following the specifications (method and values) of the Clinical and Laboratory Standards Institute7 and, more recently, of the European Committee on Antimicrobial Susceptibility Testing.8
Risk factorsThe following risk factors for infection were included: Immunosuppression: when the patient has received treatment that reduces resistance to infection (chemotherapy, radiation, corticosteroid therapy for prolonged periods of time or at high doses) or has sufficiently advanced disease to suppress the host defenses against infection (leukemia or lymphoma). Neutropenia: a neutrophil count of less than 500 cells per ml. Immune deficiency: when the patient has been diagnosed with human immunodeficiency virus (HIV) infection or some other congenital or acquired immune deficiency. Colonization or infection by a multiresistant pathogen: including methicillin-resistant Staphylococcus aureus (S. aureus) (MRSA), vancomycin resistant enterococcus, Pseudomonas aeruginosa (P. aeruginosa) resistant to three or more families of antibiotics, Acinetobacter baumannii (A. baumannii) resistant to imipenem, and extended spectrum beta-lactamase producing (ESBL) enterobacteria, defined as the identification of any of the above pathogens during patient admission to the ICU.
Measures of incidenceFor each of the studied infections (pneumonias or urinary infections or bacteremias) we estimated the cumulative incidence and the incidence density. The cumulative incidence is calculated by dividing the number of infections by the total of patients meeting the inclusion criteria, and is expressed as a percentage. The incidence density in turn is calculated by dividing the number of infections by the total days of exposure to the risk device, and is expressed as the number of infections per 1000 days of exposure. The days of exposure to the invasive devices were calculated globally for all the patients admitted during the monitorization period, according to the criteria of the NNIS.9 To this effect we performed a daily registry of the patients with MV, urethral catheter, arterial catheter and central venous catheter (including pulmonary artery catheters, parenteral nutrition, hemodialysis, and those equipped with reservoirs). For each of them we calculated the ratio of use, defined as the ratio between the number of days of use of each invasive technique and the days of risk (days of stay). In order to calculate the ratio of vascular catheters, we registered as instrumentation days the sum of days of central venous catheters and arterial catheters. Lastly, for calculating the incidence density of secondary bacteremia, we registered the total number of days of stay in the ICU.
Consumption of antimicrobialsWe registered all the antimicrobials used during the stay in the ICU, classifying them according to treatment indication: prophylaxis, treatment of community-acquired infection, treatment of nosocomial infection acquired outside the ICU, and treatment of nosocomial infection acquired in the ICU.
Statistical analysisData collection was carried out using ENVIN-ICU on a web server with access on the Internet. The database (in SQL server) is located in the same server. The program is equipped with safety mechanisms that oblige the introduction of variables defined as basic and which prevent the introduction of illogical values. Qualitative variables were described with the percentage distribution of each of the categories, while quantitative variables were reported as the mean and standard deviation in the case of a normal distribution, and as the median when otherwise. Comparison of the different variables according to the presence of one or more of the controlled infections was made for qualitative variables by using the chi-squared test (χ2). In the case of ordinal variables (categorized age or APACHE II score) we also calculated χ2 for linear trend. Logistic regression analysis was applied to identify the variables independently related to one of the controlled infections, including those variables which yielded p<0.01 in the univariate analysis. The accepted statistical significance level was 5% (p<0.05).
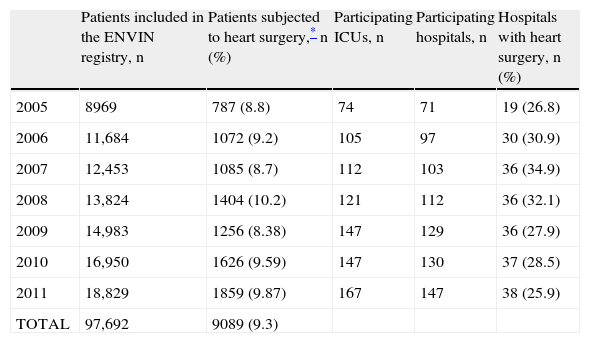
ResultsA total of 97,692 patients were included over the 7 years of the study, of which 9089 (9.3%) were POHS. The number of POHS included each year and the number of hospitals and ICUs that contributed cases to this subgroup of patients are reported in Table 1. While the proportion of hospitals with POHS did not increase, the proportion of POHS included in the registry was seen to increase from 8.8% in the year 2005 to 9.9% in the year 2011 (p<0.001).
Classification of the patients included in the ENVIN-HELICS registry in each of the controlled years.
| Patients included in the ENVIN registry, n | Patients subjected to heart surgery,* n (%) | Participating ICUs, n | Participating hospitals, n | Hospitals with heart surgery, n (%) | |
| 2005 | 8969 | 787 (8.8) | 74 | 71 | 19 (26.8) |
| 2006 | 11,684 | 1072 (9.2) | 105 | 97 | 30 (30.9) |
| 2007 | 12,453 | 1085 (8.7) | 112 | 103 | 36 (34.9) |
| 2008 | 13,824 | 1404 (10.2) | 121 | 112 | 36 (32.1) |
| 2009 | 14,983 | 1256 (8.38) | 147 | 129 | 36 (27.9) |
| 2010 | 16,950 | 1626 (9.59) | 147 | 130 | 37 (28.5) |
| 2011 | 18,829 | 1859 (9.87) | 167 | 147 | 38 (25.9) |
| TOTAL | 97,692 | 9089 (9.3) |
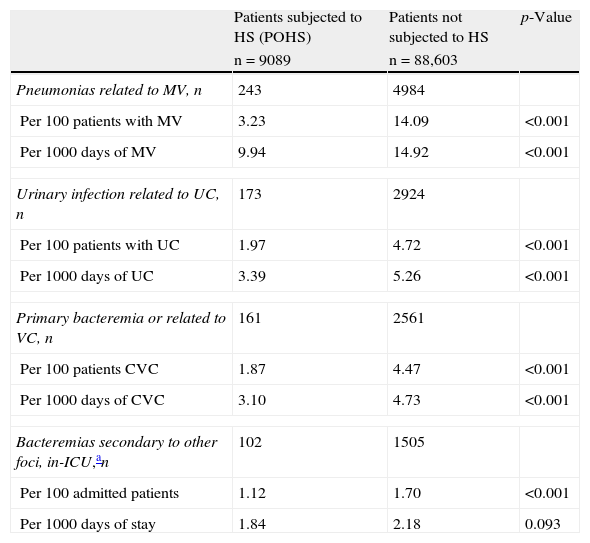
We identified one or more infections related to invasive devices and/or secondary bacteremias in a total of 440 POHS (4.8%). The rates of the controlled infections are shown in Table 2, differentiating between patients with or without heart surgery. All the infections were significantly less frequent among the POHS.
Invasive device related infection rates in the population of postoperative heart surgery patients and in the global patients included in the ENVIN-HELICS registry, between the years 2005 and 2011.
| Patients subjected to HS (POHS) | Patients not subjected to HS | p-Value | |
| n=9089 | n=88,603 | ||
| Pneumonias related to MV, n | 243 | 4984 | |
| Per 100 patients with MV | 3.23 | 14.09 | <0.001 |
| Per 1000 days of MV | 9.94 | 14.92 | <0.001 |
| Urinary infection related to UC, n | 173 | 2924 | |
| Per 100 patients with UC | 1.97 | 4.72 | <0.001 |
| Per 1000 days of UC | 3.39 | 5.26 | <0.001 |
| Primary bacteremia or related to VC, n | 161 | 2561 | |
| Per 100 patients CVC | 1.87 | 4.47 | <0.001 |
| Per 1000 days of CVC | 3.10 | 4.73 | <0.001 |
| Bacteremias secondary to other foci, in-ICU,an | 102 | 1505 | |
| Per 100 admitted patients | 1.12 | 1.70 | <0.001 |
| Per 1000 days of stay | 1.84 | 2.18 | 0.093 |
HS: heart surgery; VC: vascular catheter; CVC: central venous catheter; POHS: postoperative heart surgery patients; UC: urethral catheter; MV: mechanical ventilation.
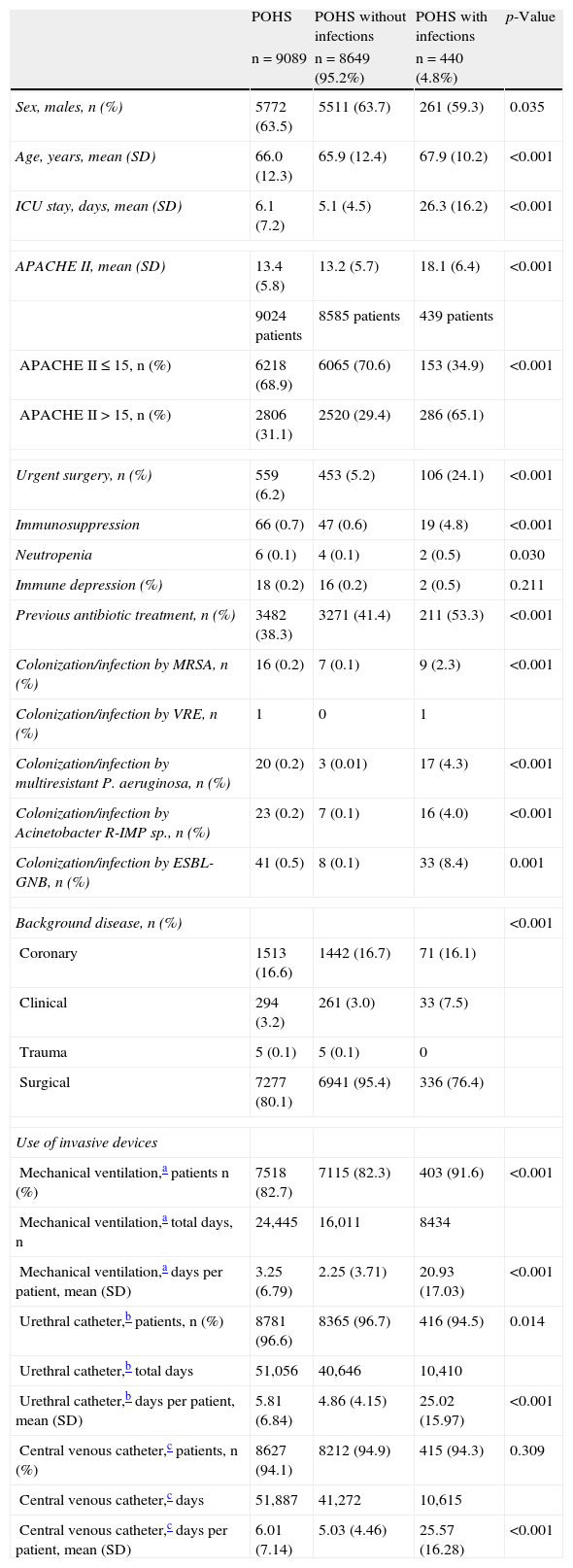
The demographic characteristics, background disease, severity markers, risk factors, days of stay in the ICU and utilization of invasive devices among the POHS according to the presence or absence of infection related to invasive devices and/or bacteremia acquired in the ICU are shown in Table 3. The logistic regression analysis identified the following individual risk factors for the development of new infection: ICU stay (odds ratio [OR] 1.18; 95%CI 1.16–1.20; p<0.001), the APACHE II score upon admission to the ICU (OR 1.05; 95%CI 1.03–1.07; p<0.001), emergency surgery (OR 1.67; 95%CI 1.13–2.47; p<0.010), previous antibiotic treatment (OR 1.38; 95%CI 1.04–1.83; p=0.025), and colonization by P. aeruginosa (OR 18.25; 95%CI 3.74–89.06; p<0.001) or extended spectrum beta-lactamase producing (ESBL) enterobacteria (OR 16.97; 95%CI 5.4–53.2; p<0.001).
Characteristics of POHS admitted to the ICU, according to the presence of one or more infections related to invasive devices and/or bacteremias secondary to other foci.
| POHS | POHS without infections | POHS with infections | p-Value | |
| n=9089 | n=8649 (95.2%) | n=440 (4.8%) | ||
| Sex, males, n (%) | 5772 (63.5) | 5511 (63.7) | 261 (59.3) | 0.035 |
| Age, years, mean (SD) | 66.0 (12.3) | 65.9 (12.4) | 67.9 (10.2) | <0.001 |
| ICU stay, days, mean (SD) | 6.1 (7.2) | 5.1 (4.5) | 26.3 (16.2) | <0.001 |
| APACHE II, mean (SD) | 13.4 (5.8) | 13.2 (5.7) | 18.1 (6.4) | <0.001 |
| 9024 patients | 8585 patients | 439 patients | ||
| APACHE II≤15, n (%) | 6218 (68.9) | 6065 (70.6) | 153 (34.9) | <0.001 |
| APACHE II>15, n (%) | 2806 (31.1) | 2520 (29.4) | 286 (65.1) | |
| Urgent surgery, n (%) | 559 (6.2) | 453 (5.2) | 106 (24.1) | <0.001 |
| Immunosuppression | 66 (0.7) | 47 (0.6) | 19 (4.8) | <0.001 |
| Neutropenia | 6 (0.1) | 4 (0.1) | 2 (0.5) | 0.030 |
| Immune depression (%) | 18 (0.2) | 16 (0.2) | 2 (0.5) | 0.211 |
| Previous antibiotic treatment, n (%) | 3482 (38.3) | 3271 (41.4) | 211 (53.3) | <0.001 |
| Colonization/infection by MRSA, n (%) | 16 (0.2) | 7 (0.1) | 9 (2.3) | <0.001 |
| Colonization/infection by VRE, n (%) | 1 | 0 | 1 | |
| Colonization/infection by multiresistant P. aeruginosa, n (%) | 20 (0.2) | 3 (0.01) | 17 (4.3) | <0.001 |
| Colonization/infection by Acinetobacter R-IMP sp., n (%) | 23 (0.2) | 7 (0.1) | 16 (4.0) | <0.001 |
| Colonization/infection by ESBL-GNB, n (%) | 41 (0.5) | 8 (0.1) | 33 (8.4) | 0.001 |
| Background disease, n (%) | <0.001 | |||
| Coronary | 1513 (16.6) | 1442 (16.7) | 71 (16.1) | |
| Clinical | 294 (3.2) | 261 (3.0) | 33 (7.5) | |
| Trauma | 5 (0.1) | 5 (0.1) | 0 | |
| Surgical | 7277 (80.1) | 6941 (95.4) | 336 (76.4) | |
| Use of invasive devices | ||||
| Mechanical ventilation,a patients n (%) | 7518 (82.7) | 7115 (82.3) | 403 (91.6) | <0.001 |
| Mechanical ventilation,a total days, n | 24,445 | 16,011 | 8434 | |
| Mechanical ventilation,a days per patient, mean (SD) | 3.25 (6.79) | 2.25 (3.71) | 20.93 (17.03) | <0.001 |
| Urethral catheter,b patients, n (%) | 8781 (96.6) | 8365 (96.7) | 416 (94.5) | 0.014 |
| Urethral catheter,b total days | 51,056 | 40,646 | 10,410 | |
| Urethral catheter,b days per patient, mean (SD) | 5.81 (6.84) | 4.86 (4.15) | 25.02 (15.97) | <0.001 |
| Central venous catheter,c patients, n (%) | 8627 (94.1) | 8212 (94.9) | 415 (94.3) | 0.309 |
| Central venous catheter,c days | 51,887 | 41,272 | 10,615 | |
| Central venous catheter,c days per patient, mean (SD) | 6.01 (7.14) | 5.03 (4.46) | 25.57 (16.28) | <0.001 |
ESBL-GNB: extended spectrum beta-lactamase producing (ESBL) enterobacteria-gram negative bacilli; VRE: vancomycin resistant enterococcus; POHS: postoperative heart surgery patients; R: resistant to 3 or more families of antibiotics; R-IMP; resistant to imipenem; MRSA: methicillin-resistant Staphylococcus aureus; ICU: Intensive Care Unit.
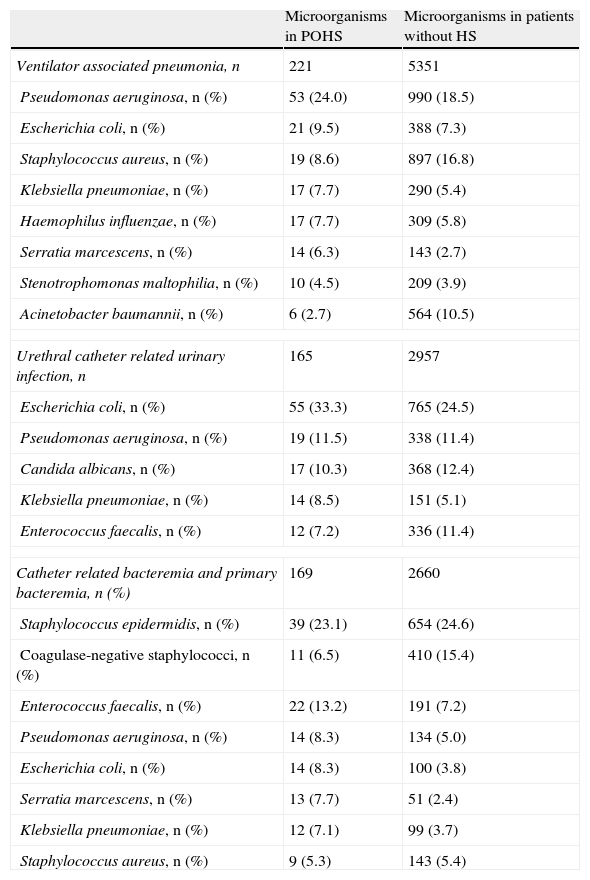
We identified 555 microorganisms in the infections related to invasive devices among the POHS. Table 4 describes the main causal pathogens in the controlled infections on a comparative basis between patients with and without heart surgery. In the case of VAP, both subgroups showed a predominance of P. aeruginosa, while the POHS showed a comparatively lesser frequency of infections produced by S. aureus and A. baumannii. In UCI and PB-VC, Escherichia coli and Staphylococcus epidermidis, respectively, predominated in both groups.
Most frequent microorganisms in each of the controlled infections in the patients subjected to heart surgery and those included in the ENVIN-HELICS registry between the years 2005 and 2011.
| Microorganisms in POHS | Microorganisms in patients without HS | |
| Ventilator associated pneumonia, n | 221 | 5351 |
| Pseudomonas aeruginosa, n (%) | 53 (24.0) | 990 (18.5) |
| Escherichia coli, n (%) | 21 (9.5) | 388 (7.3) |
| Staphylococcus aureus, n (%) | 19 (8.6) | 897 (16.8) |
| Klebsiella pneumoniae, n (%) | 17 (7.7) | 290 (5.4) |
| Haemophilus influenzae, n (%) | 17 (7.7) | 309 (5.8) |
| Serratia marcescens, n (%) | 14 (6.3) | 143 (2.7) |
| Stenotrophomonas maltophilia, n (%) | 10 (4.5) | 209 (3.9) |
| Acinetobacter baumannii, n (%) | 6 (2.7) | 564 (10.5) |
| Urethral catheter related urinary infection, n | 165 | 2957 |
| Escherichia coli, n (%) | 55 (33.3) | 765 (24.5) |
| Pseudomonas aeruginosa, n (%) | 19 (11.5) | 338 (11.4) |
| Candida albicans, n (%) | 17 (10.3) | 368 (12.4) |
| Klebsiella pneumoniae, n (%) | 14 (8.5) | 151 (5.1) |
| Enterococcus faecalis, n (%) | 12 (7.2) | 336 (11.4) |
| Catheter related bacteremia and primary bacteremia, n (%) | 169 | 2660 |
| Staphylococcus epidermidis, n (%) | 39 (23.1) | 654 (24.6) |
| Coagulase-negative staphylococci, n (%) | 11 (6.5) | 410 (15.4) |
| Enterococcus faecalis, n (%) | 22 (13.2) | 191 (7.2) |
| Pseudomonas aeruginosa, n (%) | 14 (8.3) | 134 (5.0) |
| Escherichia coli, n (%) | 14 (8.3) | 100 (3.8) |
| Serratia marcescens, n (%) | 13 (7.7) | 51 (2.4) |
| Klebsiella pneumoniae, n (%) | 12 (7.1) | 99 (3.7) |
| Staphylococcus aureus, n (%) | 9 (5.3) | 143 (5.4) |
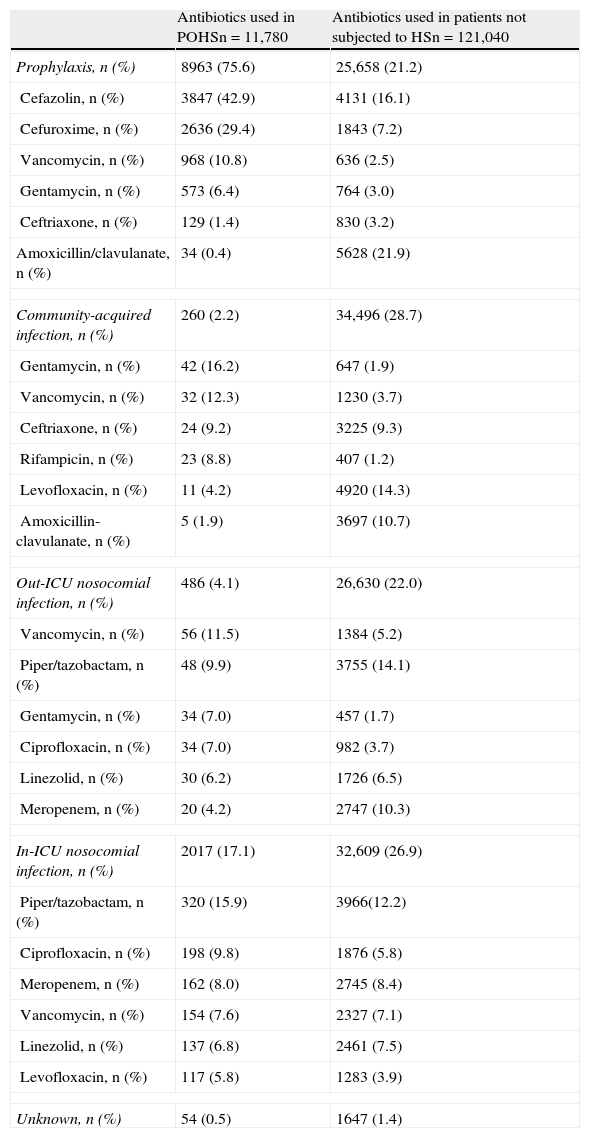
A total of 132,820 antimicrobials were used in the 97,692 patients included in the registry, and of these, 11,780 (8.7%) were used in POHS (1.29 antimicrobials per postoperative heart surgery patient). The distribution of the most extensively used antimicrobials among the POHS is shown in Table 5 according to reason for prescription. Of note in these patients is the predominance of antimicrobial use for prophylactic purposes (75.6%), particularly cefazolin (42.9%), cefuroxime (29.4%) and vancomycin (10.8%).
Reasons for use and most frequently administered antibiotics in postoperative heart surgery patients and in the rest of patients included in the ENVIN-HELICS registry between the years 2005 and 2011.
| Antibiotics used in POHSn=11,780 | Antibiotics used in patients not subjected to HSn=121,040 | |
| Prophylaxis, n (%) | 8963 (75.6) | 25,658 (21.2) |
| Cefazolin, n (%) | 3847 (42.9) | 4131 (16.1) |
| Cefuroxime, n (%) | 2636 (29.4) | 1843 (7.2) |
| Vancomycin, n (%) | 968 (10.8) | 636 (2.5) |
| Gentamycin, n (%) | 573 (6.4) | 764 (3.0) |
| Ceftriaxone, n (%) | 129 (1.4) | 830 (3.2) |
| Amoxicillin/clavulanate, n (%) | 34 (0.4) | 5628 (21.9) |
| Community-acquired infection, n (%) | 260 (2.2) | 34,496 (28.7) |
| Gentamycin, n (%) | 42 (16.2) | 647 (1.9) |
| Vancomycin, n (%) | 32 (12.3) | 1230 (3.7) |
| Ceftriaxone, n (%) | 24 (9.2) | 3225 (9.3) |
| Rifampicin, n (%) | 23 (8.8) | 407 (1.2) |
| Levofloxacin, n (%) | 11 (4.2) | 4920 (14.3) |
| Amoxicillin-clavulanate, n (%) | 5 (1.9) | 3697 (10.7) |
| Out-ICU nosocomial infection, n (%) | 486 (4.1) | 26,630 (22.0) |
| Vancomycin, n (%) | 56 (11.5) | 1384 (5.2) |
| Piper/tazobactam, n (%) | 48 (9.9) | 3755 (14.1) |
| Gentamycin, n (%) | 34 (7.0) | 457 (1.7) |
| Ciprofloxacin, n (%) | 34 (7.0) | 982 (3.7) |
| Linezolid, n (%) | 30 (6.2) | 1726 (6.5) |
| Meropenem, n (%) | 20 (4.2) | 2747 (10.3) |
| In-ICU nosocomial infection, n (%) | 2017 (17.1) | 32,609 (26.9) |
| Piper/tazobactam, n (%) | 320 (15.9) | 3966(12.2) |
| Ciprofloxacin, n (%) | 198 (9.8) | 1876 (5.8) |
| Meropenem, n (%) | 162 (8.0) | 2745 (8.4) |
| Vancomycin, n (%) | 154 (7.6) | 2327 (7.1) |
| Linezolid, n (%) | 137 (6.8) | 2461 (7.5) |
| Levofloxacin, n (%) | 117 (5.8) | 1283 (3.9) |
| Unknown, n (%) | 54 (0.5) | 1647 (1.4) |
A total of 373 POHS died during the study period (4.1%). The mortality rate among those who developed one or more infections related to invasive devices was 32.2%, versus 2.9% in those without infections (p<0.001).
DiscussionOne of the main contributions of this study has been the quantification of the proportion of postoperative heart surgery patients (POHS) among the global patients admitted to the ICUs in this country. In this context, POHS represent about 10% of the total admissions with a duration of more than 24h. In this subgroup of POHS, the infections related to invasive devices (including bacteremias acquired in the ICU due to other causes) affected 4.8% of the patients–this frequency being significantly lower than in the rest of patients admitted to the ICU. The data from this study will allow Spanish ICUs that treat POHS to compare their own rates with the national rates.
Kollef et al.,1 in a prospective single hospital study, identified one or more nosocomial infections in 21% of the POHS. In comparison, 9.2% of the patients subjected to cardiothoracic surgery in a Spanish hospital presented nosocomial infections.10 These two studies were carried out over 10 years ago, and since then there have been changes in patient management that make it difficult to establish comparisons. In a multicenter European study11 conducted in the year 2007 by the European Study Group of Nosocomial Infection and the European Society of Clinical Microbiology and Infectious Diseases, with the participation of 17 ICUs from 7 countries with the control of 11,915 POHS, a total of 9.9% of the patients were found to develop one or more nosocomial infections. This same group compiled a new registry during one month in the year 2008, with the participation of 35 hospitals from 8 countries, in which the number of patients with one or more nosocomial infections was found to decrease to 4.4%12–this figure being consistent with our own results. The main differences with respect to the mentioned studies are that in our case we only controlled infections related to invasive devices and bacteremias acquired in the ICU from other foci, but not non-bacteremic infections related to surgery (superficial surgical wound infections, mediastinitis), and moreover the observation period was limited to the duration of stay in the ICU.
The POHS who developed nosocomial infection related to invasive devices had a longer stay in the ICU, though other non-controlled factors probably also contributed to the prolongation of stay (greater severity, surgical complications, comorbidities). Most POHS remain in the ICU for 2–3 days, as has been reflected by the Spanish registry of heart surgery in Intensive Care Medicine.13 In our case the mean duration of stay was 6 days – this being justified by the fact that we did not include POHS with admissions of less than 24h.
The most frequently detected infection in our POHS was VAP (9.94 episodes per 1000 days of MV)–this figure being lower than in the rest of the controlled patients (14.9 episodes per 1000 days of MV).3 Ventilator associated pneumonia was also the principal infection identified in most studies published by other authors in this subgroup of patients.1,10,11,14,15 The VAP rate in our series was lower than in another observational study carried out between the years 2003–2006 in a Spanish ICU mainly caring for postoperative heart surgery patients, and which does not participate in the ENVIN-HELICS registry. This Unit reported VAP rates of over 22 episodes per 1000 days of MV,14 while the latest European study corresponding to the year 2008 reported 13.9 episodes of VAP per 1000 days of MV.11 These discrepancies may be a result of the impact of different interventional measures adopted by Spanish ICUs starting in the year 2009, and which have significantly reduced the infections related to invasive devices in our ICUs.16,17
A European multicenter prevalence study (a single day),18 involving 42 hospitals from 13 countries, has analyzed postoperative infections in POHS. The study included 321 patients with this diagnosis, admitted on the day of monitorization (164 of which were subjected to MV), and 26.8% of them were found to have one or more nosocomial infections–especially lower airway infections (57%), followed by catheter related bacteremias (2.8%), surgical wound infections (2.2%), urinary tract infections (0.9%) and mediastinitis (0.9%). These data, which must be viewed with caution since they come from a cross-sectional study, underscore the predominance of respiratory infections in this group of patients and the low proportion of other infections not controlled in our registry. The same study also used a parallel survey to assess the degree to which VAP preventive measures were used in the participating ICUs. In this sense, few such measures were seen to be used, thus partially explaining the high rate of these infections. The introduction of orotracheal tubes with systems for the aspiration of subglottic secretions in a heart surgery ICU has been accompanied by an important decrease in its VAP rates and in the use of antimicrobials, though the final VAP rate in that Unit remains high.19
Although heart surgery protocols involve at least intubation and MV, urethral catheterization and a central venous line, some patients no longer carry some of these devices (particularly the endotracheal tube) at the time of admission to the ICU. In our study, the proportion of patients with a tracheal tube was greater in POHS than in the global national patients admitted to the ICU, though the number of days of intubation was lower. The VAP rate in POHS was also lower, thus confirming the influence of the duration of MV upon the development of VAP20 and the need to shorten the ventilation period as much as possible in order to prevent this infection.
Although most POHS received one or more antimicrobials, these were fundamentally prescribed as prophylaxis. Of note is the use of vancomycin in 9.5% of the cases of prophylactic treatment in heart surgery, since this antibiotic should be avoided as far as possible as surgical prophylaxis in order to prevent the selection of flora resistant to glycopeptides, as has occurred in other countries.21 Its use would only be justified in patients with allergy to penicillin, in those previously colonized by multiresistant grampositive cocci, or in ICUs with endemic MRSA.
The mortality rate, as well as the prolongation of stay in the ICU, was significantly greater in the patients with one or more nosocomial infections–an observation that has been reported by all studies that have examined this aspect.1,9,10 The mortality rate and duration of stay in the ICU among patients without infection are low, and lower than expected from the level of severity upon admission to the ICU (APACHE score 13). However, the mortality rate among patients with one or more nosocomial infections is about 24%, which is in the upper range of the mortality rate expected according to patient severity at the time of admission to the ICU (APACHE score 17), and the duration of stay is over three weeks. The impact of infection in this group of patients has also been examined by other Spanish investigators who have found the mortality rate in such POHS to range from 2.8 to 45.7%, with an ICU stay of 3–25.5 days, depending on the presence of VAP in the immediate postoperative period.12 Although there are no data attributing death to the presence of VAP, all measures of caution must be used to reduce and avoid these infections, as they are clearly correlated to a poorer patient prognosis.1,10,12,14,22
A limitation of this study is its multicenter design, which may cause the criteria used in defining infection to vary despite the existence of prior consensus-based definitions included in the registry manual. On the other hand, the registry did not include the analysis of other infections not related to the use of devices, such as superficial surgical wound infections and deep infections (mediastinitis), which may have influenced the consumption of antimicrobials and the patient course–though such bias was equally found in both groups of compared patients. In turn, the study analysis did not include other risk variables in this patient population (surgical complexity, surgery time, surgical complications, EuroSCORE assessment22) which would have allowed a more precise differentiation of those patients likely to develop such infections. Lastly, since this was a non-interventional observational study, the infection preventive measures were not previously standardized or controlled.
As a conclusion to this study, it can be affirmed that an important number of patients admitted to Spanish ICUs are POHS with characteristics and outcomes that differ with respect to the rest of the patients. The appearance of one or more infections has been associated with an important prolongation of stay and a considerable increase in mortality. Consequently, one of the strategies that should be applied in these patients is the prevention of infections related to hospital activities.
Conflicts of interestThe authors declare that they have no conflicts of interest.
María Carrasco, Hospital General Vall d’Hebrón (UPCC), Barcelona (658); Lisardo Iglesias, Hospital Central de Asturias (UCI HGA), Oviedo (641); Antonio Martínez-Pellús, Hospital Virgen de la Arrixaca, Murcia (616); Ángel Arenzana, Hospital Virgen de la Macarena, Seville (613); Juan Carlos Ballesteros, Hospital Clínico de Salamanca (613); Eva María Santafosta, Hospital de Bellvitge (UCC), Hospitalet de Llobregat (Barcelona) (507); José Ramón Iruretagoyena, Hospital de Cruces, Barakaldo (Bilbao) (484); Joaquín Lobo, Hospital de Navarra, Pamplona (460); Mercedes Nieto, Hospital Clínico Universitario San Carlos (Cardiovascular ICU), Madrid (424); Mercedes Barranco, Hospital Médico Quirúrgico Virgen de las Nieves (Critical Care Unit), Granada (386); César Aragón, Hospital General Carlos Haya, Malaga (330); Sandra Barbadillo, Capio Hospital General de Catalunya, Sant Cugat del Valles (Barcelona) (269); Asunción Colomar, Hospital Son Espases, Palma de Mallorca (242); Rafael Sierra, Hospital Universitario Puerta de Mar, Cádiz (236); Benito Almirante, Hospital General Vall d’Hebrón (Critical Care Unit), Barcelona (236); Nieves Carrasco, Hospital de la Princesa, Madrid (225); Miguel Ángel Pereira, Hospital Meixoeiro-C. Hosp. Universitario de Vigo (Critical Care Unit) (222); Josep Costa, Hospital de Barcelona (SCIAS) (154); Javier Ruiz, Hospital del Sagrat Cor, Barcelona (153); María del Mar Jiménez, Hospital Médico-Quirúrgico (ICU) Virgen de las Nieves, Granada (149); José Luis Romero, Hospital Universitario de Gran Canaria Dr Negrín (147); Rafael Garcés, Hospital de la Ribera, Valencia (136); Juan Carlos Pozo, Hospital Reina Sofía, Cordoba (132); Primitivo Arribas, Hospital Universitario 12 de Octubre (PCU) (115); Josep María Sirvent, Hospital Universitario Josep Trueta, Girona (112); Ricard Jordá, Clínica Rotger, Palma de Mallorca (106); Ana Gamo, Fundación Jiménez Díaz, Madrid (106); Salomé Palmero, Hospital Universitario de Canarias, La Laguna (Tenerife) (96); Gerardo Aguilar, Hospital Clínico Universitario de Valencia (Resuscitation Unit) (68); Ana María Díaz, Complexo Hospitalario Universitario de a Coruña, A Coruña (51); Fátima Martín, Clínica Moncloa, Madrid (47); José María Borrell, Clínica Palmaplanas (USP), Palma de Mallorca (40); Juan Fajardo, Clínica Santa Isabel, Seville (40); Daniel Fontaneda, Hospital de León (Polyvalent ICU) (39), Mercedes Palomar, Hospital General Vall d’Hebrón, Barcelona (35); Hospital General Universitario de Alicante (Resuscitation) (29); Hospital Militar Gomez Ulla, Madrid (29); Hospital de León (Critical Care Unit) (28).
Please cite this article as: Álvarez Lerma F, Carrasco M, Otal JJ, Palomar M, Olaechea P, Peris X, et al. Infecciones relacionadas con dispositivos invasivos después de cirugía cardiaca. Med Intensiva. 2013;37:584–592.
The members of ENVIN-HELICS Study Group who supplied the data of patients’ “postoperative of heart surgery" are listed in Appendix A.
articles

