

Drowning is regarded as a “global killer” that has not received the attention it requires.1 In Spain, drowning is responsible for 13% of global childhood mortality due to injuries and is the second most frequent cause of accidental death, after traffic accidents.2
Drowning is preventable, and recommendations of demonstrated efficacy have been established, such as the supervision of children, the presence of lifeguards, adequate information and signaling, the protection of aquatic spaces and the use of adequate flotation devices such as life vests.1–4 In countries with a strong public safeguarding tradition such as Australia, educational programs have been shown to offer positive results in terms of learning and prevention.5 However, to the best of our knowledge, no studies in Spain have analyzed the most appropriate contents and methodology for introducing the prevention of drowning in school education. We thus sought to evaluate a pilot childhood education program focused on the understanding, learning and memorization of measures that can prevent drowning.
A sample of 26 preschool children (5 years of age) from Pontevedra (Spain) were included in the study. All of them routinely visited beaches and swimming pools, but none had received any training or instructions referred to drowning.
A quasi-experimental study design was used. The participants were divided into two cohorts: a control group (CG; n=12) that received no training, and an experimental group (EG; n=14) enrolled in the drowning prevention program. The study data were anonymized and written informed consent was obtained from all the parents.
The educational material was prepared by a multidisciplinary tam of physicians, childhood educators and lifeguards. An illustrated story for children based on an imaginary 5-year-old character was chosen, entitled “Xoana goes to the swimming pool and Xoana goes to the beach” (“Xoana va a la piscina y Xoana va a la playa”). The training program lasted one week.
Two forms were designed for the evaluation of learning: one for each scenario (beach and swimming pool) (Fig. 1). Each contained safety elements (life vest, green flag, lifeguard, supervising adult, safety barrier) and potentially hazardous elements (diving, red flag, yellow flag, eating before swimming or using a float), in compliance with the corresponding scientific recommendations.1,2 Both between- (CG versus EG) and within-group analyses (CG versus CG and EG versus EG) were made at three timepoints: before training (T0), at the end of training (T1), and after one month as a memory check (T2).
 and in the swimming pool (rounded safety elements).")
The dependent variable was the result (%) referred to the right answers minus the wrong answers in each test. The following equations were used: (Σ%right answers−Σ%wrong answers=% knowledge of prevention in swimming pool) and (Σ%right answers−Σ%wrong answers=% knowledge of prevention on beach), while for the global assessment of aquatic prevention we used: ([% knowledge of prevention in swimming pool+% knowledge of prevention on beach]/2). The SPSS version 20 statistical package for Mac (IBM Corp., Armonk, NY, USA) was used for the statistical analysis. The following statistical tests were used: (1) normal data distribution was checked with the Shapiro–Wilk test; (2) within-group analyses were based on the Mann–Whitney U-test; and (3) between-group comparisons were made using the Student t-test for independent samples or the Friedman test in the absence of a normal distribution. Statistical significance was considered for p<0.05 in all cases.
The level of knowledge of these young children was seen to be low at T0 referred to both the swimming pool and the beach (percentage right answers between 6 and 37%).
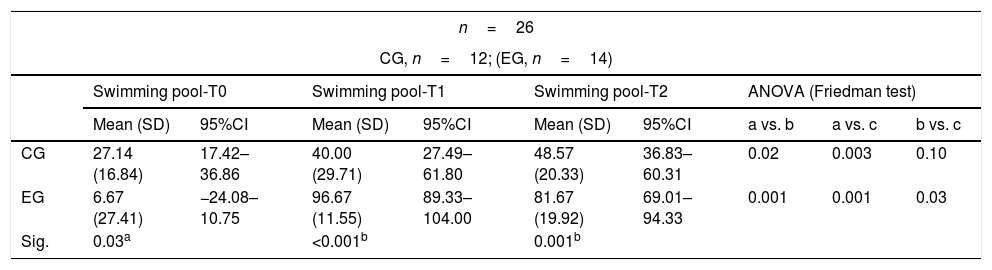
After training, the EG improved significantly at T1 versus T0 both in the swimming pool and on the beach (p<0.001). In relation to global aquatic prevention, the EG exceeded the CG by 55% (97.29±7.22 versus 42.32±22.39, respectively; p<0.001). After one month (T2), the EG continued to yield better results in both the swimming pool (p=0.001) and on the beach (p<0.001), and in relation to global aquatic prevention, the EG exceeded the CG by 41% (89.79±10.68 versus 48.39±17.15, respectively; p<0.001). In turn, the within-group analysis showed clear improvement between T0 and T1, with learning stabilization at T2 (Table 1).
Results referred to the evaluation of knowledge about the prevention of drowning in the different study phases.
| n=26 | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| CG, n=12; (EG, n=14) | |||||||||
| Swimming pool-T0 | Swimming pool-T1 | Swimming pool-T2 | ANOVA (Friedman test) | ||||||
| Mean (SD) | 95%CI | Mean (SD) | 95%CI | Mean (SD) | 95%CI | a vs. b | a vs. c | b vs. c | |
| CG | 27.14 (16.84) | 17.42–36.86 | 40.00 (29.71) | 27.49–61.80 | 48.57 (20.33) | 36.83–60.31 | 0.02 | 0.003 | 0.10 |
| EG | 6.67 (27.41) | −24.08–10.75 | 96.67 (11.55) | 89.33–104.00 | 81.67 (19.92) | 69.01–94.33 | 0.001 | 0.001 | 0.03 |
| Sig. | 0.03a | <0.001b | 0.001b | ||||||
| Beach-T0 | Beach-T1 | Beach-T2 | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Mean (SD) | 95%CI | Mean (SD) | 95%CI | Mean (SD) | 95%CI | a vs. b | a vs. c | b vs. c | |
| CG | 37.50 (23.51) | 23.92–51.08 | 44.64 (29.71) | 27.49–61.80 | 48.21 (20.72) | 36.25–60.18 | 0.26 | 0.03 | 1.00 |
| EG | 25.00 (15.08) | 15.42–34.58 | 97.92 (7.22) | 93.33–102.50 | 97.92 (7.22) | 93.33–102.50 | 0.001 | 0.001 | 1.00 |
| Sig. | 0.12a | <0.001b | <0.001b | ||||||
| GAP-T0 | GAP-T1 | GAP-T2 | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Mean (SD) | 95%CI | Mean (SD) | 95%CI | Mean (SD) | 95%CI | a vs. b | a vs. c | b vs. c | |
| CG | 32.32 (16.63) | 22.72–41.92 | 42.32 (22.39) | 29.39–55.25 | 48.39 (17.75) | 38.15–58.64 | 0.02 | 0.004 | 0.13 |
| EG | 15.83 (17.03) | 5.01–26.66 | 97.29 (6.52) | 93.15–101.44 | 89.79 (10.68) | 83.00–96.58 | 0.001 | 0.001 | 0.09 |
| Sig. | 0.02a | <0.001b | <0.001b | ||||||
ANOVA: analysis of variance; SD: standard deviation; CG: control group; EG: experimental group; 95%CI: 95% confidence interval; Sig.: statistical significance; T0: test 0 pre-training; T1: test 1 post-training; T2: test 2 one month post-training; GAP: global assessment of aquatic prevention.
Different studies indicate that the introduction of drowning prevention strategies in the educational system has positive effects in terms of recognizing drowning triggering factors at vulnerable ages.5,6 While preliminary, our data show how a simple but well oriented intervention is able to ensure learning and retaining of what has been learned over the middle term in children as young as 5 years of age. The data obtained should serve to support the design and implementation of broad and systematic school programs for reducing the incidence of drowning in our setting.
Please cite this article as: Barcala-Furelos R, Carbia-Rodríguez P, Peixoto-Pino L, Abelairas-Gómez C, Rodríguez-Núñez A. Implantación de programas educativos para prevenir ahogamientos. ¿Qué se puede hacer desde la escuela infantil? Med Intensiva. 2019;43:180–182.

