


Technological advances have played a key role over the last century in the development of humankind. Critical Care Medicine is one of the greatest examples of this revolution. Smartphones with multiple sensors constitute another step forward, and have led to the development of apps for use by both professionals and patients. We discuss their main medical applications in the field of Critical Care Medicine.
Los avances tecnológicos han sido clave en el último siglo para el desarrollo de la humanidad. La Medicina Intensiva es uno de los mayores exponentes de esta revolución. Los teléfonos inteligentes (smartphones) con múltiples sensores son un paso más en este avance y han dado lugar al desarrollo paralelo de las aplicaciones (apps) para uso tanto por profesionales como por pacientes. Comentamos las principales aplicaciones médicas en el ámbito de la Medicina Intensiva.
Technological advances have been a significant element for the evolution of mankind during the last century. Basically it has been due to the still unrecognized “computing revolution”, that has allowed us to change all areas of our society and has revolutionized Medicine. Intensive Care Medicine is one of the best examples of this revolution due to all the technologies available today for all kinds of support for organic systems.
Since the birth of mobile phones, in 1973, when the Motorola CEO, Martin Cooper made the very first phone call with a DynaTAC 8000X to his fiercest competitor, this industry has experienced an unstoppable growth. The real blooming of these technologies would occur in 2007, when charismatic Steve Jobs brought us the first generation of the iPhone®, introducing the revolutionary concept of using touch-screen technology instead of physical keyboards, changing from that moment onwards the way would we interact with these devices. The launch of the App Store followed – one repository of applications compatible with this device that provides an extra of security and reliability.
The technological advancement experienced during the last years was due to various factors that determined the great advancement of mobile and portable devices:
- •
Hardware: the high capacity of computing reached with the development of smaller and more energy efficient microchips; the blooming of smartphones that has reduced costs and made these devices a global phenomenon; and the development of different activity sensors that monitor vital signs and other biological functions—also blooming during the last year thanks to wearable devices.
- •
Software: the development of easier, safer and more user friendly-operating systems, and the development of mobile applications (apps).
- •
Conectivity: with global access to the Internet from any devices thanks to wireless (Wi-Fi) and data (3G, 4G, etc.) networks.
As it occurs in other fields, Medicine has also experienced the changes brought by this computing revolution through the vision of electronic health, eSalud or eHealth, based on information and communication technologies.
Mobile health or mHealth has potential applications in public health issues since it grants access to healthcare resources to a wide array of people, and without saturating the system since it reduces consultations, hospital stays, and healthcare costs.1 In industrialized countries it is seen as an alternative that may solve the problem of costs and access to healthcare of an increasingly ageing population, while in developing countries and thanks to the arrival of mobile technologies to these countries, it will grant access to healthcare to the majority of low income-populations who live in rural areas.
As part of the eHealth, the electronic health records (EHR) and the data collected through apps will be used and analyzed trough the so-called Big Data. It will be a game changer as it has been the case in other industries where it was implemented some time ago—like Internet browsers that offer individual results based on prior searches. Applied to healthcare it can mean the development of tools that will assist us in the clinical decision making process, in the individualization of recommendations for every patient, or in the sending of these recommendations directly to patients—thus improving clinical practice, and the quality and efficiency of healthcare.2
However, there is still a big jump between the potential benefits of this technology and its real translation into healthcare systems, with certain challenges and setbacks still unresolved today such as feasibility, reliability, stability, privacy, security and friendly use of these systems, as we will see later.
Apps and medicineNowadays, there is a great variety of applications generically related to health, some for patients and some for healthcare providers. And yet despite the great amount of apps that repositories have to offer, not many are backed by scientific evidence, not even weak evidence.
There is a group of apps oriented towards the use of these technologies by patients that try to improve health in various ways:
- •
Primary prevention: used to control blood pressure, body weight, etc.
- •
Health training: apps that help identify the signs and symptoms of different diseases so that we know when to ask for medical assistance, like the app designed by the American Heart Association on how to recognize strokes.
- •
Process to facilitate self-care and guided therapies: patient-focused apps have major implications in treatment since the patient is not a passive subject anymore in the healthcare process and acquires self-care responsibilities, which increases adherence to treatment. Today there are multiple diseases like diabetes,3 COPD,4 asthma,5 or obesity,6 or processes like smoking deshabituation,7 weight loss8 and other prevalent conditions,9 where new technologies allow us to monitor and better control these conditions, even though the evidence behind this is still scarce.10
- •
Rehabilitation: there are experiences of cardiac tele-rehabilitation after suffering a myocardial infarction,11 and also for the management of strokes the first experimental studies have been proposed, comparing tele-rehab with mobile devices and sensors monitored by therapists to conventional therapy.12 This can result in a wide use of therapies with the same aviable means, with the obvious benefit for society.
This plan can also change the actual paradigm of Medicine by allowing, in an economically feasible way, the outpatient control of patients with chronic diseases through apps certified by healthcare authorities that would guide them in the home control of their conditions and assist them on when to ask for medical assistance, which in a not so remote distant future would turn doctors into prescribers of treatments, drugs, and apps. When it comes to patients requesting admission in intensive care units, with these apps we would be able to assess their clinical situation and prior outpatient control.
Also, the arrival of new technologies brings many changes in many settings of the development of the medical profession. During the last years we have seen the blooming of smartphones both for healthcare providers and the general population.13 And even though there are too many professional health-related apps, some repositories have designed and built specific apps for the healthcare community.
Intensive care medicine and appsEven though, as we have said, due to its idyosincracy, our medical field is the most highly technified of all, its relation with mobile apps is scarce: searches in PubMed («Critical Care»[Mesh]) AND «Mobile Applications»[Mesh]) provide no results. However, there are many areas of knowledge in our medical field with experiences published in smartphones and apps—some of them created by Spanish intensive care physicians.
The repository of professional apps for our medical field is huge, and we can distinguish several groups.
Dissemination of informationMany publishing houses have apps for the distribution of their journals, with formats similar to physical journals, and with the advantages that immediate distribution and updated contents have to offer. Some of the apps from this group are the specific apps of landmark journals in our specialty such as Intensive Care Medicine, or Critical Care Medicine. Through these apps we can have access to all issues published these journals that can be bought individually or downloaded in the case we have an active subscription.
Also, there are apps we can use to search through biomedical literature databases such as PubMed/MEDLINE, PubMed on Tap (iOS), and PubMed Mobile (Android) and PubMed4Hh (Android, iOS). Some of them even let us build our own references. Also, apps such as Leer, built by QxMD (Read by QxMD, available for both platforms) let us set up individual alerts based on keywords, prominent papers based on their relevance or recommendations from other colleagues, which produces ongoing quality scientific updates.
Mendeley (available for iOS and Android) is a free app for the management of references and quotes capable of PDF format file reading. It has desktop versions for PC and Mac that also allow us to manage references and introduce bibliographic quotes in different word processors.
EndNote (iOS) is the commercial version of Thomson Reuters, available for tablets, that allows us to manage and read bibliographic quotes, and PDF files. There is also one desktop version for PC and Mac to use it with different word processors.
PharmacopoeiaWhat these apps have in common is the information they present: name of the drug, posology, pharmacokinetics, pharmacodynamics, adverse events, adjustments based on the renal or liver functions, clinical manifestations, costs, etc. Usually they are versions of drug databases built by the government, which guarantees their reliability and updating.
They are useful for specific searches as it is the case with unusual drugs used by patients, dose intervals, need for dose titration in situations of renal failure or lists of side effects.
Here are some of thes most significant ones:
- •
aempsCIMA. The Online Centre for Drug Information (CIMA, in Spanish) endorsed by the Spanish Agency of Medical Products and Medical Devices has its own app—that is free of charge, and where we can search for drugs commercially available in Spain—whether by commercial name or active ingredient. It allows us to search for authorized drugs, non-authorized drugs, or both, commercialized drugs, or non-commercialized drugs. It provides access to the technical sheet and/or label, information on the manufacturing lab, the date of commercialization, the ATC classification—anatomic, therapeutic, and chemical, and the list of clinical presentations.
- •
Medimecum®, property of rheumatologist, Dr. Luis Fernando Villa Alcázar. This is low-cost app and right now it is available for iOS devices only. It includes data available in the printed version of the same name (indications, posology, side effects, etc.) and direct access to the technical sheet of each drug as provided by the Spanish Agency of Medical Products and Medical Devices.
- •
Vademécum, property of Vidal Vademécum Spain. Part of it is free of charge and provides the same information for each drug available in its website (indications, posology, side effects, etc.) and also has payment modules (pharmacological guide, and interactions). In any case, it needs prior registration, something necessary to make consultations and inquiries of the same information through the website.
These belong to another groups of widely used apps of special relevance in the intensive care setting and of great utility at bedside care. In general, they are useful for prognostic indexes, formulae related to analytical values and infusion dose titration. And even though there are apps for single calculations, most of them include various calculations—usually classified by organs or systems. Most apps provide precise and reliable results according to one of the few papers that put these medical calculators to the test.14
The most widely used among Android users is the MediCalc® app, which is a free app in Spanish language that includes a great number of calculations and that is great for making calculation groups, thus enabling the single introduction of common variables. It does not have a specific module on intensive care and includes calculation from different severity indexes and regular classification systems that we use in our setting, such as APACHE, SOFA, qSOFA, RIFLE, etc.
Among iOS users the most valued apps are MedCalc, MedCalX, and MDCalc. They have a similar profile and are available in English language. However, MedCalc—of Swiss origin and developed by Dr. Pfiffner and Dr. Tschopp, stopped being free a long time ago, which has increased the number of downloads of the MDCalc app, commercialized by MD Aware as an app, even though it has an old tradition as an online calculator.
Other similar medical calculators are the Medimath/Mediquation Medical Calculator, Calculate by QxMD, or the CliniCalc-Medical Calculator.
Here we should also mention the UCI RenalCalc® app developed by the intensive care physician, Dr. Antoni J. Betbesé, that offers complete functionality for dose titration, velocities, pressures, etc., commony used in continuous renal replacement therapies.
Finally, we need to mention the EMRA PressorDex free app developed by the Emergency Medicine Residents’ Association (EMRA) and initially designed to make perfusion calculations with some basic treatment algorithms.
Medical informationNow we will mention apps with summaries on topics, schemes, or diagnostic algorithms. They include information that even though could be presented in other formats that combine texts, and images, consultations are easier and user-friendlier in the format of an app.
Among the specific ones, the following are the most widely used:
- •
SanfordGuide is the app format of the most famous guide of infectious diseases in English language. It is a fee-for-service app and can only be acquired through the general module of infectious diseases and/or HIV/AIDS, and hepatitis.
- •
The Antibiotic Therapeutic Guide (iOS and Android) is an app designed and created by the Commission of Hospital Infections, Prophylaxis and Antibiotic Policy from the Hospital Son Espases (Palma de Mallorca, Spain). It provides guides and diagnostic and therapeutic algorithms with general aspects over the use of antimicrobians, guides of empirically supported treatment and prevention manuals. It also provides calculators capable of measuring infectious processes, web resources and access to the commission blog.
- •
Sepsis Clinical Guide. It provides clinical information and tools used in the diagnosis and management of sepsis and septic shocks. It is updated with definitions from the third conference on sepsis,15 has a new quick-SOFA index for the rapid evalutation of sepsis, treatment measures from the Surviving Sepsis Campaign and results from the ARISE,16 ProCESS,17 and ProMISE18 trials. This app is designed to be used by physicians and other healthcare providers managing critically ill patients.
- •
iTox (iOS and Android), creaded by pharmacologist, Dr. Antonio Dueñas-Laita. It is a fee-for-service app and is in Spanish language. It has a large database with specifics on action mechanisms, signs and symptoms, diagnosis, treatment and prognosis of poisonings.
- •
EchoCalc is basically a free ultrasound manual developed by the British Society of Echocardiography describing the different slices and normal values of ultrasound measurements.
- •
Uptodate includes reviews of over 10,000 topics in constant discussion. Even though it requires subscription, the great variety of topics it includes, and its primarily practical and concise profile have made it a very popular app, and many health institutions that have already subscribed now offer access from their website.
Certain apps are also available including some of the aforementioned functionalities. Many all-in-one-apps include one more or less large database with different topics of discussion. They are very popular:
- •
Medscape: it is a free app whose contents have all been designed in English language; it has been developed by WebMD, is available for iOS and Android, and requires prior registration for use. It has numerous functions: pharmacopoeia, pharmacological interactions, disease thematic index, one system to be able to identify prescription tablets, one medical calculator, medical proceedings, etc. Also, Medscape provides one specific version for intensive care medicine with clinical data, discussions, continuing medical education seminars, papers of interest, and news from different areas of interest of this or that medical specialty.
- •
Epocrates® (iOS and Android): it is a free app designed in English language with one drug section with one interactive module, one system for tablet identification through description and one basic section of therapeutic and diagnostic algorithms. It requires prior registration. There is also a more complete fee-for-service app including guidelines on clinical practice, one manual with diseases and another manual on alternative medicine, the ICD-10 classification, and treatment protocols on infectious diseases.
- •
Omnio (iOS and Android): it is an update of the famous Skyscape. Through one simple registration we will have easy and quick access to relevant medical information such as: medications guides, the Merck Manual, calculators, news, interaction analyser, and guidelines from the CDC, the American Diabetes Association and the National Comprehensive Cancer Network.
- •
iDoctus (iOS and Android): Spanish app for consultations and medical reference including drug databases with one interactive module, one disease thematic index, calculators, one multimedia database, and clinical cases. Its content is permanently updated, and has reliable sources such as the drug database designed by the Spanish General Council of Official Colleges of Pharmacists. Also, it has a profile based on our medical field by picking up relevant papers and information of interest.
Mobile devices, PDAs at the beginning and then smartphones like tablets, have always had the potential of storing large amounts of information such as books, notes, etc. However, this potential is more powerful in these tablets thanks to Internet connectivity and the functionality of app interaction—something of vital importance in a process of learning. Recent studies show that the students of medical schools and young attending physicians use these new technologies (in over 75 per cent), and require apps for their academic training and clinical practice,19 and this is the reason why many medical schools and residency programmes have replaced textbooks for electronic tablets in order to teach diagnoses, proceedings, and operations.20–22 And yet despite tha fact that the development of apps is growing and that we have more and more apps for the training of procedures and skills, the scientific evidence behind all this is still weak.
Diagnosis and treatmentDiagnostic tool apps have been designed to achieve precise diagnoses and treatments. Many of these apps are versions of landmark medical books for the diagnosis of diseases. Most provide information on infectious diseases, laboratory values, pathogens, differential diagnoses, treatments, etc. There is an old study from 2004 that shows that the five most widely used apps on 202 cases provide correct treatment recommendations in over 95 per cent of the cases.23 These apps are symptom-based and help the clinician order the correct lab tests or image modalities, reduce healthcare costs, and improve the patient's security.
- •
enGuardia: is a mobile tool care assistance aimed at clinicians. With over 100 diseases, differential diagnoses, and interactive algorithms, it is particularly useful for both point-of-care and urgent situations.
- •
iResus: app developed by the Resuscitation Council that allows access to the latest CPR guides and algorithms for adults, children, and newborn babies. And yet despite the fact that its use in controlled settings offered better results in CPR management,24 no further studies have been conducted that would back up its clinical use.
The use of smartphones has proven benefitial in intensive care settings because of the reduced risk of medical errors following the immediate communication they provide with respect to pagers.25 Smartphones provide other ways of communication different than voicemails and text messages such as emails, multimedia messages, videoconferences, and other messaging apps. Whichever app we choose, they have improved communication in different settings such as the experiences published by surgeons,26 transplant coordinators,27 or emergency services.28
Smartphones and apps enable inter-patient communication through the use of regular apps,29 or apps specifically developed for communication purposes without linguistic barriers, such as the Patient Communicator app by SCCM, created by the Society of Critical Care Medicine, that eliminates all linguistic barriers (bidirectional communication in 19 different languages), while offering the possibility of choosing what part of your body hurts and what the intensity of sensations such as pain, itches, nausea, etc., really is, which in turn helps reduce anxiety and pain, and increase the levels of satisfaction.
Clients for hospital information systemsThese apps enable access to different hospital information systems such as electronic health records (EHR), electronic medical records (EMR), or systems of digital storage, transfer, and download of radiological images, such as Osirix HD, and are flexible so we can use our devices to have safe access to our patients’ information from anywhere, and at anytime.
ResearchThe collection of data from studies, clinical trials, etc., through apps may help standardize the collection of variables and their online registration while reducing mistakes, facilitating analysis and providing greater data confidentiality.
This has a real translation since one of the largest manufacturers of smartphones and software today—Apple Inc., has developed an open-code platform designed and focused on medical and healthcare research: ResearchKit. Once authorized by the user, the apps operating under this platform (available in appstore.com/researchkit) allow us to use different health-related data captured by both the mobile wearable device and any third-party devices. This gives us the possibility to collect, in a short period of time, a great deal of information and better knowledge on prevalent diseases such as Parkinson's disease (mPower), the type and duration of epileptic seizures (Epiwatch), the follow-up of ashma (Asthma Health), CET (Concussion Tracker), COPD (StopCOPD), etc. All this with a very important focus on privacy, giving users absolute control of the information they have access to from each app and the visualization of data shared at anytime. Thanks to this technology, we can select more patients, conduct more efficient follow-ups, with fewer losses and lower costs, which empowers and gives more meaning to the studies already conducted.30
From a more practical standpoint, we should talk about the ICU Trials app by ClinCalc (iOS and Android)—one quick-reference app for the intensive care physician, including short summaries and key points from the main clinical trials of Medicine.
InnovationAmong the most innovative apps, we should mention the one developed by Airstrip Technologies LP, that lets us do real time visualizations of the patients’ vital signs both through our smartphone, and through the latest versions of smartwatches.
Also, we should discuss here Lumify, by Philips®, one app with one transducer connected to the phone capable of turning the phone into one point-of-care ultrasound system—one of the most relevant medical advances of 2015.
Capstesia is an app for both iOS and Android platforms developed by GalenicApp® (Vitoria-Gasteiz, Spain) that digitalizes the invasive blood pressure curves provided by all types of monitors (Fig. 1). It provides us with pulse pressure variations of the digitalized curves, the mean of the maximum curve slopes (dPmax/dt), and estimates of the cardiac output through a proprietary algorithm. It estimates derived values (cardiac index, systolic volume index, peripheral vascular resistance, peripheral vascular resistance index), and tables and tendencies across time that grant us access to advanced monitoring with lower costs than that of specific monitors.
 showing the haemodynamic calculations made from the photocopy of one invasive arterial blood pressure seen in the lower side of the image.")
This app is still in the process of clinical validation though some studies have already validated it in simulation settings.31
Security and risksObviously, serious risks are associated with the use of these technologies in today's society of information.
PrivacyThe users’ collection of data through multiple apps increases the chances of exposing sensitive information, both personal and healthcare-related information.
Many times, the user does not even know how the app operates internally, what services it connects to, what the protocols it uses, etc. This is why its use is based on confidence only, which, obviously, is not enough for users or institutions to adopt these technologies without a strict review of security in data storage and transfer. As a matter of fact, today there are apps that yet despite the fact that they are certified or endorsed by public services or scientific societies, are not as reliable as expected, as it shows one study conducted during 6 months among 79 apps with certifications of being clinically safe and trustworthy, according to the United Kingdom National Health Service that confirmed that 88 per cent of the apps transferred information online (of which 66 per cent were not encrypted) while 100 per cent of the apps did not encrypt the personal information stored in the device32—a potential risk of exposing sensitive personal information.
In view of the above on the development of apps, the hallmark for generating trust both for users and the healthcare systems should be a clear policy of privacy and security for the management of data collected locally (in the device) that are transferred and stored remotely (in public and private servers), while abiding by the applicable law in matters of privacy, ethical regulations, and needs for medical information.
Health risksYet despite the fact that software programmes come with a number of processes and debuggers, the risks of malfuncioning, errors, etc., are a reality. This can be a vital risk for patients, as one study on apps for the resuscitation of burn-injured patients confirmed, where 13 out of the 32 apps analyzed showed errors in the estimation of fluid therapy with respect to the total body surface area burned.33
This is why institutions such as the European Commission and the U.S. Food and Drug Administration (FDA) have taken measures and come up with a guide of recommendations for the industry that puts apps in the same level as any other drug or medical device.34,35 even though the FDA puts a special emphasis on apps that have a greater impact on human health (specified in its Annex C), like apps capable of turning a smartphone into a medical device (e.g., apps that use sensors for ECG measuring purposes), apps capable of connecting to a medical device to control how the device operates (e.g., apps that change the configuration of an infusion pump), or apps capable of showing, transferring, converting, or storing patients’ data from one connected device (e.g., apps that transfer patients’ data to central nursing stations).
Microbiological threatDue to the high levels of implementation of this technology, smartphones have turned into potential biological threats since they are carriers of pathogens in the clinical setting, as it has already been confirmed.36 They can have the role of harbouring and transmitting multi-drug resistant organisms and be a source of bacterial cross-contamination due to hand-face interactions, especially in the ICU settings of newborn babies and adults.37
Today, we do not know of any legislation, recommendation, or institutional protocol that can guarantee the proper cleaning of smartphones and other electronic devices to further avoid any bacterial contaminations. As a matter of fact, the manufacturers of electronic devices explicitely warn against the use of aggressive products like the disinfectants used in the cleaning of surfaces.
At least for the time being, it seems reasonable to follow the directions on hand sanitation until new prevention strategies are implemented that take into account the use of these devices in clinical settings and keep the devices covered with disposable bags. The use of different types of towels, not all of them allowed by the manufacturers of these devices though, has been a topic of discussion in certain pilot studies,38 yet for now research in this field is insufficient. The development of waterproof, washable smartphones, or phones covered by antibacterial nanomaterials, and the use of ultraviolet radiation stand as the new measures in the fight against bacterial contamination.
Loss of contact with the patientThis quick access to clinical history, including former health records, image modalities, etc., has evident advantages, but we should also take into account the time physicians spend in front of their computers and laptops – a powerful source of distraction with potential disastrous effects39 that pushes anamnesis and physical exploration to a place they should have never gone in the first place.
AdvantagesNot all are setbacks with these new technologies. Among the advantages of using apps and smartphones, we should mention the following:
- •
Quick access to information: immediate searches through database indexation.
- •
Portability: inherent to the very mobile device and providing a great deal of updated information and bedside care of optimal quality.
- •
Segurity: debugged and verified apps provide further security to the process of drug titration and administration, to the performance of proceedings, etc.
- •
User-friendliness: the familiarity that the routine use of the actual operating systems brings allows the development of intuitive, easy to use apps that require a short period of learning.
- •
Networking access: The Internet powers mobile apps.
- •
Data storage: even though it is one of the greatest threats to security, if done correctly data storage can be a great advancement for data access and preservation.
Apps are part of the so-called «new Medicine» of tomorrow that is already a reality today as we have been seeing over the last few years with more and more quantity and quality pilot projects and preliminary, descriptive studies that are laying the foundations for the potential uses of these tools to be translated, in the future, into safe and reliable clinical and educational settings.
Also this translates into great advances and threats that should be considered challenges.
The use of apps and the interaction with the information collected by other health-related electronic registration systems will individualize and optimize both clinical practice, and the quality and efficiency of primary care.
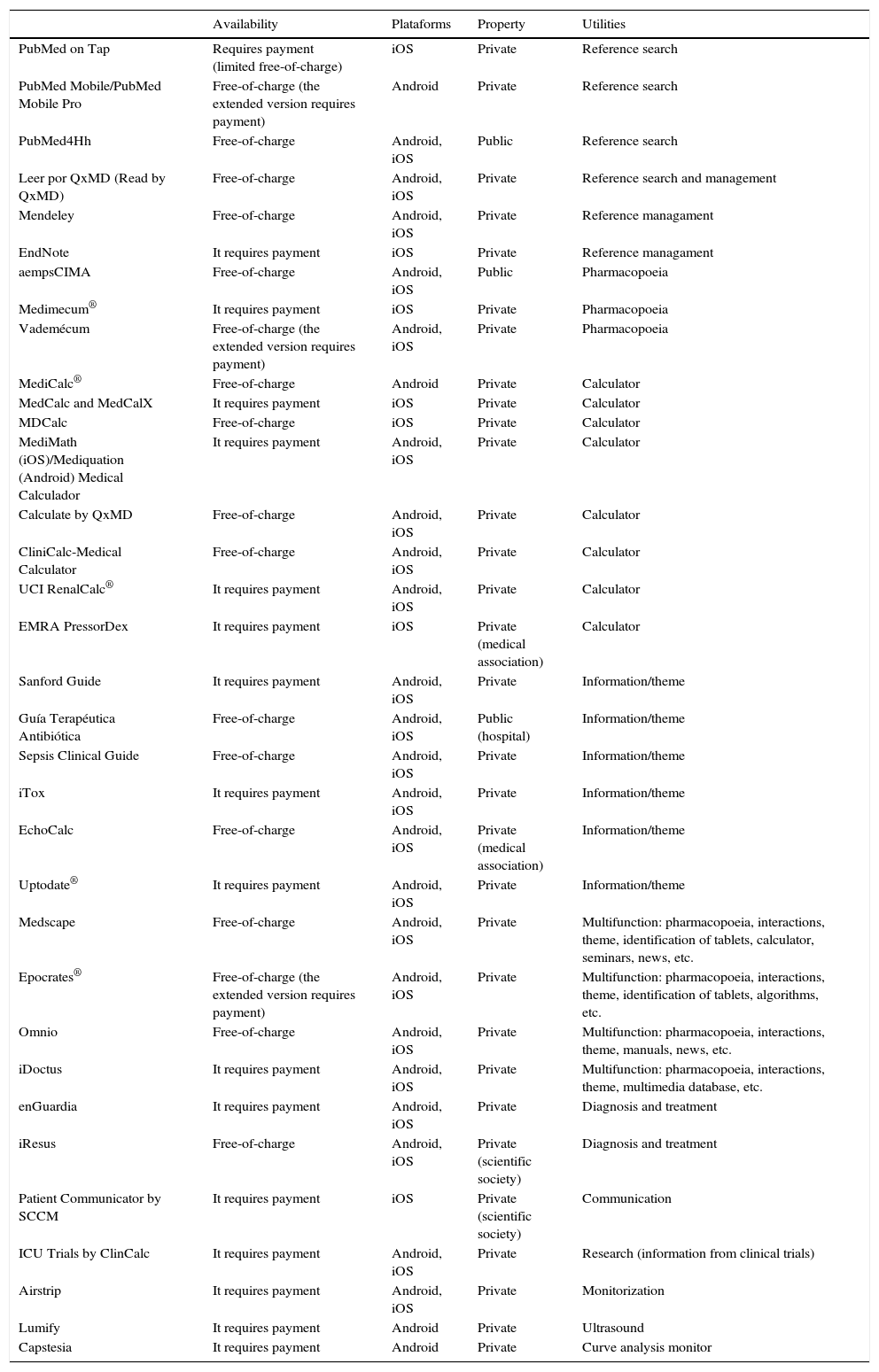
The entities that develop these apps, the healthcare systems and scientific societies, should create a legal framework, a security framework and studies showing its efficiency so that they become useful, reliable, efficient, and certified tools within the healthcare systems (Table 1).
Most widely used apps.
| Availability | Plataforms | Property | Utilities | |
|---|---|---|---|---|
| PubMed on Tap | Requires payment (limited free-of-charge) | iOS | Private | Reference search |
| PubMed Mobile/PubMed Mobile Pro | Free-of-charge (the extended version requires payment) | Android | Private | Reference search |
| PubMed4Hh | Free-of-charge | Android, iOS | Public | Reference search |
| Leer por QxMD (Read by QxMD) | Free-of-charge | Android, iOS | Private | Reference search and management |
| Mendeley | Free-of-charge | Android, iOS | Private | Reference managament |
| EndNote | It requires payment | iOS | Private | Reference managament |
| aempsCIMA | Free-of-charge | Android, iOS | Public | Pharmacopoeia |
| Medimecum® | It requires payment | iOS | Private | Pharmacopoeia |
| Vademécum | Free-of-charge (the extended version requires payment) | Android, iOS | Private | Pharmacopoeia |
| MediCalc® | Free-of-charge | Android | Private | Calculator |
| MedCalc and MedCalX | It requires payment | iOS | Private | Calculator |
| MDCalc | Free-of-charge | iOS | Private | Calculator |
| MediMath (iOS)/Mediquation (Android) Medical Calculador | It requires payment | Android, iOS | Private | Calculator |
| Calculate by QxMD | Free-of-charge | Android, iOS | Private | Calculator |
| CliniCalc-Medical Calculator | Free-of-charge | Android, iOS | Private | Calculator |
| UCI RenalCalc® | It requires payment | Android, iOS | Private | Calculator |
| EMRA PressorDex | It requires payment | iOS | Private (medical association) | Calculator |
| Sanford Guide | It requires payment | Android, iOS | Private | Information/theme |
| Guía Terapéutica Antibiótica | Free-of-charge | Android, iOS | Public (hospital) | Information/theme |
| Sepsis Clinical Guide | Free-of-charge | Android, iOS | Private | Information/theme |
| iTox | It requires payment | Android, iOS | Private | Information/theme |
| EchoCalc | Free-of-charge | Android, iOS | Private (medical association) | Information/theme |
| Uptodate® | It requires payment | Android, iOS | Private | Information/theme |
| Medscape | Free-of-charge | Android, iOS | Private | Multifunction: pharmacopoeia, interactions, theme, identification of tablets, calculator, seminars, news, etc. |
| Epocrates® | Free-of-charge (the extended version requires payment) | Android, iOS | Private | Multifunction: pharmacopoeia, interactions, theme, identification of tablets, algorithms, etc. |
| Omnio | Free-of-charge | Android, iOS | Private | Multifunction: pharmacopoeia, interactions, theme, manuals, news, etc. |
| iDoctus | It requires payment | Android, iOS | Private | Multifunction: pharmacopoeia, interactions, theme, multimedia database, etc. |
| enGuardia | It requires payment | Android, iOS | Private | Diagnosis and treatment |
| iResus | Free-of-charge | Android, iOS | Private (scientific society) | Diagnosis and treatment |
| Patient Communicator by SCCM | It requires payment | iOS | Private (scientific society) | Communication |
| ICU Trials by ClinCalc | It requires payment | Android, iOS | Private | Research (information from clinical trials) |
| Airstrip | It requires payment | Android, iOS | Private | Monitorization |
| Lumify | It requires payment | Android | Private | Ultrasound |
| Capstesia | It requires payment | Android | Private | Curve analysis monitor |
Apps are becoming tools of the new technologies of information that have a great potential in all settings of the medical field, and offer promising opportunities to improve the scope and quality of the healthcare services.
Conflicts of interestsWe the authors declare that while conducting this paper there were no conflicts of interests linked whatsoever.
Please cite this article as: Iglesias-Posadilla D, Gómez-Marcos V, Hernández-Tejedor A. Apps y Medicina Intensiva. Med Intensiva. 2017;41:227–236.

