



Respiratory physiotherapy, including the management of invasive mechanical ventilation (MV) and noninvasive mechanical ventilation (NIV), is a key supportive intervention for critically ill patients. MV has potential for inducing ventilator-induced lung injury (VILI) as well as long-term complications related to prolonged bed rest, such as post-intensive care syndrome and intensive care unit acquired weakness. Physical and respiratory therapy, developed by the critical care team, in a timely manner, has been shown to prevent these complications. In this pathway, real-time bedside monitoring of changes in pulmonary aeration and alveolar gas distribution associated with postural positioning, respiratory physiotherapy techniques and changes in MV strategies can be crucial in guiding these procedures, providing safe therapy and prevention of potential harm to the patient. Along this path, electrical impedance tomography (EIT) has emerged as a new key non-invasive bedside strategy free of radiation, to allow visualization of lung recruitment. This review article presents the main and potential applications of EIT in relation to physiotherapy techniques in the ICU setting.
La fisioterapia respiratoria, es una pieza fundamental en la intervención clínica del paciente crítico. Dentro de las funciones clínicas del fisioterapeuta respiratorio, se puede contar la participación en el manejo de la ventilación mecánica invasiva (VM) como no invasiva (VNI), la terapia física y la ejecución de técnicas de fisioterapia respiratoria a nivel del tórax. La evidencia actual ha demostrado que mayor tiempo en VM se pudiese asociar potencialmente a daño pulmonar (VILI) y complicaciones musculares periféricas como debilidad muscular adquirida en la unidad de cuidados intensivos y potencial síndrome post cuidados intensivos. En esta vía la terapia física y respiratoria, implementada por el equipo de cuidados críticos, ha demostrado prevenir estas complicaciones. Es por esto, que la monitorización en tiempo real - que permita visualizar cambios en la aireación pulmonar y la distribución del gas alveolar, asociados a cambios posturales, técnicas de fisioterapia respiratoria y la aplicación de diferentes estrategias de VM - pudiese ser crucial guiando la seguridad de estos procesos clínicos. De esta forma la tomografía por impedancia eléctrica (TIE) emerge como una técnica novedosa, no invasiva y libre de radiación, que permite la monitorización pulmonar al borde de la cama del enfermo crítico guiando y potenciando diversos actos clínicos para el mejor tratamiento del usuario en la unidad crítica. Es por esto que esta revisión presenta las potenciales aplicaciones de la TIE en la relación a las técnicas de fisioterapia respiratoria en el paciente crítico.
Monitoring of the respiratory system is crucial for managing critically ill patients in the intensive care unit (ICU).1 Advancements in imaging techniques have allowed for better understanding of mechanical ventilation (MV) and recruitability of the lungs.2 One such technique is the electrical impedance tomography (EIT), which was developed several decades ago and enables real-time evaluation of pulmonary ventilation without the need for invasive procedures.3 Nevertheless, despite its long history of development, the clinical and research applications of EIT in critically ill patients are still not fully understood.4 Furthermore, little is known about its potential use in assessing rehabilitation, mobilization, and respiratory physiotherapy.5
The purpose of this narrative review is to provide an overview of the physical principles, mode of use, ventilatory indices, and clinical utilities of EIT in the context of respiratory physiotherapy.
Physical and operating principles of EITRespiratory monitoring using EIT allows for real-time visualization of lung air distribution at the patient’s bedside. EIT is a noninvasive and radiation-free device. EIT works placing an electrode belt around the thorax, typically between the 4th or 5th intercostal space, depending on the device used. This location provides a representative view of the pulmonary field without interference from large blood vessels or the diaphragm muscle. The electrodes in the belt deliver a low-amplitude, high-frequency electric current sequentially, and changes in resistance during the respiratory cycle are calculated based on these measurements. Additionally, a reference electrode is placed 10 cm away from the electrode belt to ensure consistent electrical potential for accurate measurements.6
Changes in resistances occur due to the elongation and thinning of the alveolar septum, which obstructs the passage of electric current. Studies have reported that resistivity increases by more than 200% during deep breaths.7 Numerous studies have demonstrated a close correlation between aeration changes detected by EIT and aeration assessed by computed tomography scan (CT), that is considered the gold standard for lung aeration assessment.8
At the end of a complete sequence of electrical injection, voltage measurements are used to generate an image using specific reconstruction algorithms. Each image corresponds to a specific period recorded as a baseline for all patients. After reconstruction, the images are projected onto a 32 × 32-pixel matrix, where each pixel represents the variation in air resistance during a defined time interval.9
The main advantage of EIT over other imaging methods is its high temporal resolution, as it can generate up to 50 images per second (50 frames). This allows for the immediate evaluation of phenomena such as lung recruitment and derecruitment in response to changes in position or secretions suctioning, for instance.6 Moreover, either for real time or offline analysis of the data, each image can be divided into regions of interest (ROIs). Within each ROI, it is possible to early visualize the baseline aeration and any dynamic change associated, as shown in percentage, and afterword to extract the plethysmography curve or resistance curve, where the amplitude corresponds to changes in air volume and the frequency corresponds to the respiratory rate. This enables the objective assessment of ventilation changes between different regions and facilitates the comparison of aeration behavior between the left and right lung or between the upper and lower regions. The waveform reflects changes in local electrical impedance. Ventilation or the action of the heart and lung perfusion induce periodic fluctuations in the signal, and current devices incorporate a frequency filter to separate the perfusion component from the overall plethysmography signal. Point changes may be caused by factors such as an overall increase in gas volume due to increased positive end-expiratory pressure (PEEP) during mechanical ventilation10 or by changes in patient position5 EIT waveforms may also show artifacts originating, for example, from body motion or interference with some medical devices, but these can often be eliminated by offline processing of the signal and data,11 with pacemakers currently being the only clinical device that is considered exclusion criteria for EIT use.
In EIT, a color map is used to visually identify aeration zones. Lighter shades of blue indicate areas with significant impedance changes, corresponding to well-aerated lung zones. Darker shades of blue represent areas with less impedance change, indicating less aeration in those lung zones,10 see Fig. 1.

Representation of changes in impedance and aeration. Legend: the lighter blue color corresponds to an area that has shown a large impedance change. Correlative, therefore, to a well-ventilated lung area. The darker blue shade color represents areas with less impedance change. Correlative to a lung zone with less aeration. Regions of interest are observed in quadrants or in layers. Each of the regions of interest expresses a percentage of the total tidal impedance change.
Considering the aforementioned characteristics, EIT allows for the specific assessment of phenomena related to air distribution within a lung region. It can be used, for example, to guide processes during mechanical ventilation, ventilatory support, intensive kinesiology procedures such as functional mobilization, and manual techniques of respiratory physiotherapy, among others.10
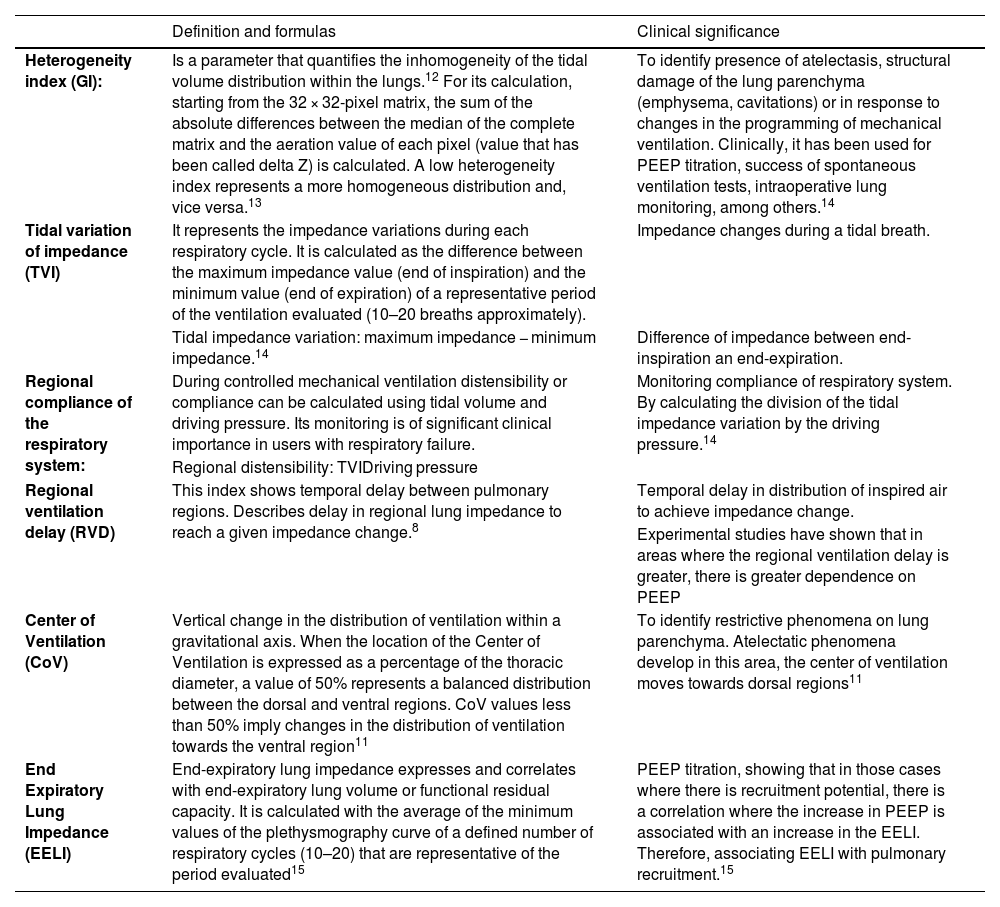
Indices that can be evaluated with the EITSeveral indices can be assessed by the EIT. These indices include the heterogeneity index or global inhomogeneity index, tidal variation of impedance, regional compliance of the respiratory system, regional ventilation delay, center of ventilation, and end expiratory lung impedance. Table 1 summarizes the definitions, usefulness, and associated formulas of all these indices.
Indices that can be evaluated with the EIT.
| Definition and formulas | Clinical significance | |
|---|---|---|
| Heterogeneity index (GI): | Is a parameter that quantifies the inhomogeneity of the tidal volume distribution within the lungs.12 For its calculation, starting from the 32 × 32-pixel matrix, the sum of the absolute differences between the median of the complete matrix and the aeration value of each pixel (value that has been called delta Z) is calculated. A low heterogeneity index represents a more homogeneous distribution and, vice versa.13 | To identify presence of atelectasis, structural damage of the lung parenchyma (emphysema, cavitations) or in response to changes in the programming of mechanical ventilation. Clinically, it has been used for PEEP titration, success of spontaneous ventilation tests, intraoperative lung monitoring, among others.14 |
| Tidal variation of impedance (TVI) | It represents the impedance variations during each respiratory cycle. It is calculated as the difference between the maximum impedance value (end of inspiration) and the minimum value (end of expiration) of a representative period of the ventilation evaluated (10–20 breaths approximately). | Impedance changes during a tidal breath. |
| Tidal impedance variation: maximum impedance − minimum impedance.14 | Difference of impedance between end-inspiration an end-expiration. | |
| Regional compliance of the respiratory system: | During controlled mechanical ventilation distensibility or compliance can be calculated using tidal volume and driving pressure. Its monitoring is of significant clinical importance in users with respiratory failure. | Monitoring compliance of respiratory system. By calculating the division of the tidal impedance variation by the driving pressure.14 |
| Regional distensibility: TVIDriving pressure | ||
| Regional ventilation delay (RVD) | This index shows temporal delay between pulmonary regions. Describes delay in regional lung impedance to reach a given impedance change.8 | Temporal delay in distribution of inspired air to achieve impedance change. |
| Experimental studies have shown that in areas where the regional ventilation delay is greater, there is greater dependence on PEEP | ||
| Center of Ventilation (CoV) | Vertical change in the distribution of ventilation within a gravitational axis. When the location of the Center of Ventilation is expressed as a percentage of the thoracic diameter, a value of 50% represents a balanced distribution between the dorsal and ventral regions. CoV values less than 50% imply changes in the distribution of ventilation towards the ventral region11 | To identify restrictive phenomena on lung parenchyma. Atelectatic phenomena develop in this area, the center of ventilation moves towards dorsal regions11 |
| End Expiratory Lung Impedance (EELI) | End-expiratory lung impedance expresses and correlates with end-expiratory lung volume or functional residual capacity. It is calculated with the average of the minimum values of the plethysmography curve of a defined number of respiratory cycles (10–20) that are representative of the period evaluated15 | PEEP titration, showing that in those cases where there is recruitment potential, there is a correlation where the increase in PEEP is associated with an increase in the EELI. Therefore, associating EELI with pulmonary recruitment.15 |
To date, the role of the intensive care physiotherapist in promoting functional mobility and assisting in the respiratory therapy of critically ill subjects has become relevant within the intensive care team. Physiotherapy has been shown to reduce functional complications in survivors of the ICU. Particularly, respiratory physiotherapy techniques can promote mucociliary clearance and lung recruitment. These techniques include high flow oxygen therapy (HFOT), noninvasive mechanical ventilation (NIV), invasive mechanical ventilation, and assistance in the weaning process from mechanical ventilation as well as the physical rehabilitation of critically ill subjects.12
Respiratory physiotherapyRespiratory physiotherapy techniques aim to expand the thorax to promote lung recruitment and prevent the retention of bronchial secretions and atelectasis.13
Respiratory physiotherapy can promote airway permeabilization.14 It also includes techniques such as:
- •
Postural drainage (positioning subject in lateral decubitus to facilitate drainage of bronchial secretion using the force of gravity12);
- •
Manual lung hyperinflation (using a manual rebreathing bag connected to a flow of oxygen. A pressure is applied to the bag that is capable of generating pressure peaks of up to 40 cmH2O12);
- •
Ventilator lung hyperinflation (this maneuver is performed in controlled mechanical ventilation, doing six breaths per minute with an inspiratory slow flow of 20 L/min, then an inspiratory pause of 2 s, followed by hyperinflation by increasing tidal volume by 200 mL until peak airway pressure of 30 cmH2O12);
- •
Percussion (percussing with palm of hand rhythmically on the affected lung segment12);
- •
Vibro-compression (fast rhythmic movements with high intensity to cause vibration at the bronchial level. Performed by hand open on the thorax applying pressure);
- •
Compression techniques should achieve a difference higher than 33 L/min between peak expiratory flow and peak inspiratory flow (PEF–PIF)15); and
- •
Aspiration techniques (direct aspiration of the secretion into the endotracheal tube).
The evidence on the use of respiratory physiotherapy techniques in subject with ARDS is still controversial.4 In this sense, EIT could result in a guide for the application of such maneuvers in subjects with high risk and alveolar instability. Recent evidence has shown that EIT – looking at center of ventilation and end-expiratory lung impedance (EELI) – is a tool that can guide physiotherapy at the bedside of the critically ill subject, not only to compare lung aeration pre versus post therapy, but also to obtain a real-time guide to alveolar gas gain and distribution.13,16
In spontaneously ventilated subjects with ARDS, there is a potential risk for spontaneous ventilation-induced lung injury (P-SILI).17 This risk could be exacerbated by lung expansion maneuvers performed by the physiotherapist. By performing a simple calibration consisting of executing 10 breaths inside a calibration balloon and using the tidal variation of impedance differences, it is possible to determine with EIT the tidal volume mobilized by the subject, even during non-invasive respiratory support or respiratory physiotherapy maneuvers in spontaneously breathing subjects. This could help prevent P-SILI and ensure a safer process of respiratory physiotherapy.18
Body position and physical therapyThe body position of critically ill subjects affects ventilation and can lead to decreased lung volume and hypoxemia.19 Physical therapy can help mitigate the negative effects associated with bed rest.20 For example, the application of HFOT in postoperative abdominal surgery subjects placed in a semi-sitting position in bed – inclined at 45° – has been shown to increase EELI as evaluated by EIT, compared to conventional oxygen therapy.25 In addition, in subjects undergoing mechanical ventilation with mild to moderate ARDS, higher positioning such as sitting on the edge of the bed, bipedal standing, walking, and other functional activities have been found to increase EELI and oxygenation without the need to increase PEEP or FiO2,5 as shown in Fig. 2.
Noninvasive mechanical ventilation
Alteration in pulmonary aeration is easily recognized by EIT through three indexes: the heterogeneity index,21 the variation of tidal impedance22 and pulmonary impedance at the end of expiration.23
NIV, which in the last 20 years has played a crucial role in the management of ventilatory failure in the emergency room and in the ICU, is considered the support of choice in 80% of exacerbations associated with chronic cardiac and respiratory failure and the first line technique to relief subject’s symptoms in 40% of cases,24,25 thus providing a positive pressure that increases EELI. Specifically, a clinical trial found that survivors increased EELI of 50% as compared with non-survivors, where the EELI increased only by 24%.26
High flow oxygen therapyThe use of HFOT can be helpful to prevent intubation and invasive MV in subjects with hypoxemia and a mild to moderate increase of work of breathing.27 In healthy young people, without increased ventilatory work, an increase in EELI is generated when comparing ventilation in high flow nasal cannula device as compared with room air. Several groups of researchers seek to find a predictor index that determines the need for intubation when using HFOT, through evaluation with EIT, without finding differences between subjects who presented a favorable clinical response to high-flow oxygen therapy compared to those who did not.28 Recently, an asymmetric cannula, designed with a smaller diameter tip and a larger diameter tip, has been approved for clinical use, resulting in an overall 30%–40% increase in total cross-sectional area compared to a conventional interface of the same size.29 This clinical trial used EIT to compare the effects on EELI of conventional nasal cannula versus asymmetric cannula.
Specific clinical situations in subjects under mechanical ventilationVisualization of air trappingRecent evidence reports the possibility of visualizing trapped air though EIT – which would constitute intrinsic PEEP – during acute obstructive events in users with exacerbated chronic obstructive pulmonary disease under invasive mechanical ventilation. This by means of visualization regional end-expiratory flow. Indeed, it is possible to diagnose air trapping by EIT, as well as to guide clinical therapeutics such as the execution of aerosol therapy.30 In that way EIT could visualize effective nebulization to provide efficient inhalation delivery of the drug, increasing, if necessary, the effective dose to reach the distal airways.31
Assessment of spontaneous ventilationThe transition from controlled ventilation, under sedation, to spontaneous or partially controlled ventilatory modalities is a challenge that the clinician faces, especially in situations where connection to mechanical ventilation is associated with respiratory failure. In this sense, EIT allows observing how in injured lungs, a “pendelluft” phenomenon can be generated; movement of air within the lung from non-dependent to dependent regions, without any change in tidal volume, generating dangerous mechanical tension in the dorsal areas, all this caused by spontaneous breathing during mechanical ventilation, at the wrong time.32
In this sense, in patients with ARDS, “pendelluft” phenomenon associated with the onset of spontaneous ventilation has been demonstrated. This phenomenon presented an independent association with the increase of specific inflammatory biomarkers related to lung injury induced by mechanical ventilation, such as interleukin (IL)-8, IL-18, and Caspase-1.33
Spontaneous breathing trial testThe process of liberation from MV, known as weaning, is a critical event that involves removing the endotracheal tube and invasive MV support. The success or failure of weaning from MV can greatly impact the morbidity and mortality of critically ill subjects. The spontaneous breathing trial (SBT) is a testing process to determine if a subject can ventilate without support. However, there is currently no consensus on the best technique to define the success or failure of extubation. Multi-modal monitoring is crucial in this pathway to aid in clinical decision-making.34
In some cases, respiratory fatigue, indicated by a loss of EELI at EIT, has been observed within the first five minutes of SBT. Patients who experience this exhaustion phenomenon also tend to have a higher rate of heterogeneity.34
If the heterogeneity index is greater than 41.5, it is not recommended to extubate the subject as it is associated with a failure rate of 87.5%, with a sensitivity of 60.9%. For subjects with an initial heterogeneity index of >41.5, the spontaneous ventilation test should be avoided to prevent failures in 87.5% of cases, with a sensitivity of 60.9%. This method could be used as a detection method to support decision-making.35 EIT seems more precise in predicting successful weaning compared to functional parameters of gas exchange or respiratory mechanics.36 Indeed, during spontaneous breathing, the variation of tidal impedance is significantly reduced, indicating increased respiratory fatigue.34
Alveolar recruitment maneuverAlveolar recruitment maneuvers (ARM) are a procedure used in MV in selected cases in subjects with acute respiratory failure or ARDS, where alveolar instability is observed. Many techniques of respiratory physiotherapy can promote alveolar recruitment, and protocolized physiotherapy sessions often include ARMs. The goal of ARM is to decrease lung collapse, improve oxygenation, lung compliance, and increase functional residual capacity.37
It is crucial to determine the lung’s recruitment capacity to avoid overdistension and potential VILI.38 In this context, EIT plays an important role in providing real-time information on the behavior of lung ventilation and its homogeneity during the maneuver. This information can be used to optimize the application of PEEP and tailor the strategy to each subject’s characteristics.
A recent study published by Jonkman et al.39 describes in a cohort of subjects diagnosed with moderate to severe ARDS by COVID-19, the use of EIT to define alveolar recruitment potential and PEEP titration. The study analyzed optimal PEEP, regional distribution of collapse and overdistension, regional distribution of ventilation, recruitment/inflation ratio (R/I), respiratory mechanics, hemodynamics, gas exchange, and recruitment capacity. The authors concluded that EIT is important and feasible in establishing individualized PEEP values, optimizing protective mechanical ventilation The authors conclude the importance and feasibility of EIT to establish an individualized PEEP value according to the characteristics of distensibility and alveolar recruitment of each subject, thus optimizing protective mechanical ventilation.39
Recently, the combination of EIT and esophageal balloon has been used to provide individualized mechanical ventilation support and protection in subjects on mechanical ventilation.35 In addition, a recent systematic review has concluded that the use of EIT is a useful imaging technique that provides safety when performing a PEEP titration maneuver.40
ConclusionsEIT is a promising non-invasive tool that could guide clinical strategies for respiratory physiotherapy maneuvers, such as to identify the right time to switch from controlled to assisted ventilation and spontaneous breathing in the context of weaning from MV, PEEP titration, visualization of acute phenomena such as atelectasis, pleural effusion, pneumothorax, and assessment of subject ability to cough. EIT offers advantages over traditional monitoring tools, including non-invasiveness, radiation-free imaging, and dynamic monitoring. This real-time guidance will also make it possible to observe the distribution of alveolar gas within the lungs, which will lead to safer physiotherapy.
Authors’ contributionRA writing first draft. All authors substantial contribution in conception and design, interpretation of literature, revision for critical important intellectual content, editing, approval of the version submitted. DB supervision, writing, editing.
FundingNone.
Conflicts of interestNone.
None.

