



Edited by: Alberto García-Salido - Pediatric Intensive Care Unit, Hospital Infantil Universitario Niño Jesús, Madrid, Spain
Last update: May 2024
More infoLower respiratory tract infections (LRTI) are a common cause of acute respiratory failure (ARF) in children and a common reason for admission into Pediatric Intensive Care Units (PICU). Syncytial respiratory virus (SRV)—the main causative agent behind acute bronchiolitis and pneumonia in children under two years of age—has a very particular seasonal epidemiological pattern, with maximum incidence peaks in the months of November and February.1 Although LRTI often have a benign evolution, there are times when they can occur more severely, requiring PICU admission in 10%–20% of children hospitalized due to LRTI.2
The disease caused by SARS-CoV-2 (COVID-19), declared a worldwide pandemic back in March 2020, is the cause of severe ARF in adults; however, it affects children in a smaller proportion, usually causing milder manifestations. The COVID-19 pandemic has put tremendous pressure on the healthcare system and changed the epidemiology of other causes of hospitalization in both children and adults.3,4
This is an observational, retrospective study, where we analyze the epidemiology of ARF admissions due to LRTI in a PICU during the COVID-19 pandemic (from March 1st, 2020 through February 15th, 2021) compared to 4 previous epidemic seasons (from September 1st, 2016 through February 29th, 2020), the pre-pandemic period. This is a mixed PICU—pediatric and neonatal—that provides healthcare to 105,320 children between the ages of 0 and 14 years with a median of 400 admission/year (20% neonatal disease, 20% critical pediatric patients, 28% postoperative patients, and 32% admissions to perform techniques and procedures).
LRTI was considered when the clinical signs were characterized by cough, tachypnea, and respiratory distress with pathologic lung auscultation preceded by flu-like symptoms with or without fever. We only included patients whose reason for PICU admission was ARF due to LRTI diagnosed with acute bronchiolitis, acute viral bronchitis, status asthmaticus, viral or bacterial pneumonia, and pertussis. Regarding the patients with status asthmaticus, we only included those with bronchial asthma diagnosis who showed signs suggesting LRTI.
The demographic characteristics, clinical data, and etiological agent were all collected. The study was approved by the Drug Research Ethics Committee of our center.
During the study period, a total of 1780 patients were admitted to the PICU, 363 (20.4%) due to pediatric critical illness, 182 of whom were admissions due to respiratory causes. A total of 161 ARF admissions were analyzed due to LRTI.
We saw a significant reduction in the rate of ARF admissions at the PICU due to LRTI, from 50% (149/298) in the pre-pandemic period down to 18.5% (12/65) during the pandemic (OR = 0,23; IC95%, 0,12–0,44; p < 0,001). The rate of admissions was estimated on the number of pediatric critical patients, excluding admissions due to neonatal, postoperative illness and those aimed to perform techniques or procedures.
The medians of age and weight were higher in the group of children admitted during the COVID-19 pandemic compared to the pre-pandemic group. The main diagnoses in the pre-pandemic period were bronchiolitis (39.6%), and acute viral bronchitis (32.9%) while during the pandemic no admissions due to bronchiolitis were reported.
Viral agent detection was performed using the molecular diagnosis technique with nasopharyngeal swab specimen collection in all the patients. During the pre-pandemic period, the SRV was the most common causative agent (50.3%) followed by entero/rhinovirus (38.3%). SRV caused 89.8% of all cases of acute bronchiolitis while the entero/rhinovirus was detected more frequently in acute viral bronchitis (43%), and status asthmaticus (53%). In seven patients (4.7%) no causative agent was found (5 with a diagnosis of acute bronchitis, and 2 with a diagnosis of status asthmaticus). Co-infection by 2 or more viruses was reported in 36.7% of the cases.
During the COVID-19 pandemic, the viruses detected were entero/rhinovirus (50%) and human metapneumovirus (16.7%). A total of 5 patients had status asthmaticus, in 4 of them the entero/rhinovirus was isolated compared to 1 patient in whom the human metapneumovirus was seen as the causative agent. A total of 2 cases of viral pneumonia were seen (due to entero/rhinovirus and SARS-CoV-2), and 1 case of acute viral bronchitis with co-infection of 2 different viruses (entero/rhinovirus, and metapneumovirus). No causative agent was isolated in 2 patients (16.7%).
Regarding LRTI of bacterial etiology, 13 patients (8.7%) were admitted due to bacterial pneumonia in the pre-pandemic period, and one (8.3%) during the COVID-19 pandemic. Also, a case of pertussis was reported during the pandemic.
Fig. 1 shows the number of ARF admissions to the PICU on a monthly basis due to LRTI and the frequency of detection of respiratory viruses.

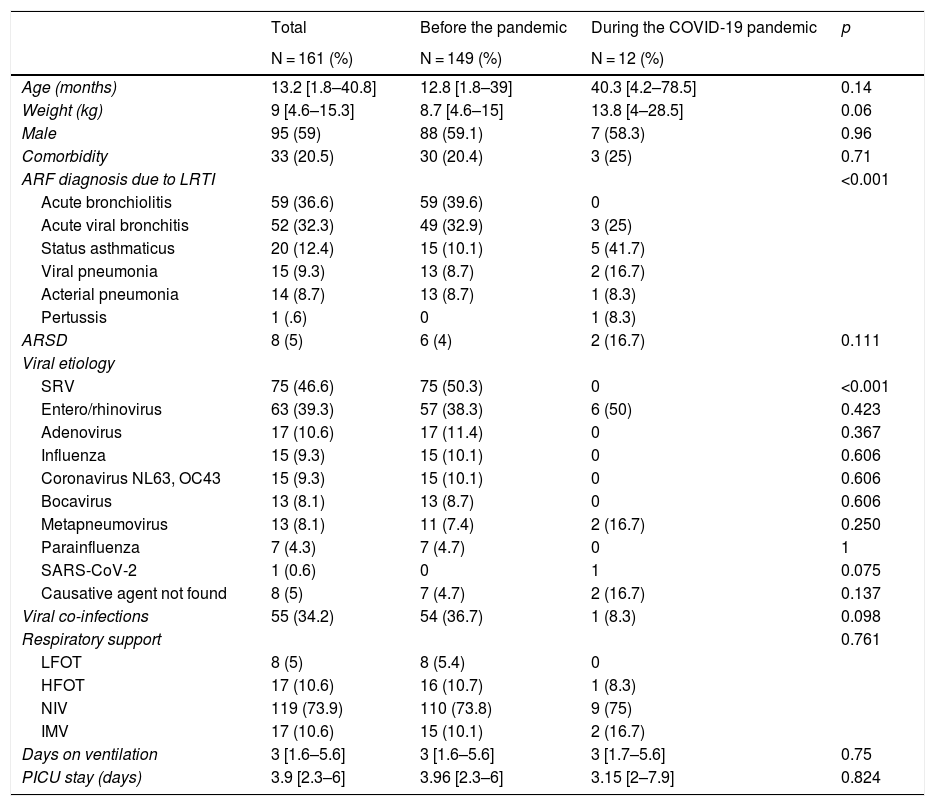
The use of ventilation support was similar in the 2 study periods. During the pre-pandemic period, 73% required non-invasive ventilation (NIV) while 10.1% required invasive mechanical ventilation. On the other hand, during the pandemic, NIV was used in 75% of the cases and 2 patients (16.7%) were intubated, 1 with pneumonia due to COVID-19. Table 1 shows the patients’ demographic and clinical characteristics during the 2 study periods.
Demographic and clinical characteristics of patients during the 2 study periods.
| Total | Before the pandemic | During the COVID-19 pandemic | p | |
|---|---|---|---|---|
| N = 161 (%) | N = 149 (%) | N = 12 (%) | ||
| Age (months) | 13.2 [1.8–40.8] | 12.8 [1.8–39] | 40.3 [4.2–78.5] | 0.14 |
| Weight (kg) | 9 [4.6–15.3] | 8.7 [4.6–15] | 13.8 [4–28.5] | 0.06 |
| Male | 95 (59) | 88 (59.1) | 7 (58.3) | 0.96 |
| Comorbidity | 33 (20.5) | 30 (20.4) | 3 (25) | 0.71 |
| ARF diagnosis due to LRTI | <0.001 | |||
| Acute bronchiolitis | 59 (36.6) | 59 (39.6) | 0 | |
| Acute viral bronchitis | 52 (32.3) | 49 (32.9) | 3 (25) | |
| Status asthmaticus | 20 (12.4) | 15 (10.1) | 5 (41.7) | |
| Viral pneumonia | 15 (9.3) | 13 (8.7) | 2 (16.7) | |
| Acterial pneumonia | 14 (8.7) | 13 (8.7) | 1 (8.3) | |
| Pertussis | 1 (.6) | 0 | 1 (8.3) | |
| ARSD | 8 (5) | 6 (4) | 2 (16.7) | 0.111 |
| Viral etiology | ||||
| SRV | 75 (46.6) | 75 (50.3) | 0 | <0.001 |
| Entero/rhinovirus | 63 (39.3) | 57 (38.3) | 6 (50) | 0.423 |
| Adenovirus | 17 (10.6) | 17 (11.4) | 0 | 0.367 |
| Influenza | 15 (9.3) | 15 (10.1) | 0 | 0.606 |
| Coronavirus NL63, OC43 | 15 (9.3) | 15 (10.1) | 0 | 0.606 |
| Bocavirus | 13 (8.1) | 13 (8.7) | 0 | 0.606 |
| Metapneumovirus | 13 (8.1) | 11 (7.4) | 2 (16.7) | 0.250 |
| Parainfluenza | 7 (4.3) | 7 (4.7) | 0 | 1 |
| SARS-CoV-2 | 1 (0.6) | 0 | 1 | 0.075 |
| Causative agent not found | 8 (5) | 7 (4.7) | 2 (16.7) | 0.137 |
| Viral co-infections | 55 (34.2) | 54 (36.7) | 1 (8.3) | 0.098 |
| Respiratory support | 0.761 | |||
| LFOT | 8 (5) | 8 (5.4) | 0 | |
| HFOT | 17 (10.6) | 16 (10.7) | 1 (8.3) | |
| NIV | 119 (73.9) | 110 (73.8) | 9 (75) | |
| IMV | 17 (10.6) | 15 (10.1) | 2 (16.7) | |
| Days on ventilation | 3 [1.6–5.6] | 3 [1.6–5.6] | 3 [1.7–5.6] | 0.75 |
| PICU stay (days) | 3.9 [2.3–6] | 3.96 [2.3–6] | 3.15 [2–7.9] | 0.824 |
ARDS, acute respiratory distress syndrome; HFOT, high flow oxygen therapy; IMV, invasive mechanical ventilation; LFOT, low flow oxygen therapy; NIV, non-invasive ventilation.
The categorical variables were expressed as absolute values and percentages (%), and the quantitative ones as median and interquartile range [IQR]. The Mann–Whitney–Wilcoxon test was used to compare the continuous variables while Fisher’s exact test was used to compare the qualitative variables. Significance level ≤0,05.
This study shows a significant decrease in the rate of PICU admissions due to ARF following LRTI during the COVID-19 pandemic. The measures implemented to reduce SARS-CoV-2 transmission such as hand sanitation, use of the face mask, and social distancing, have probably contributed to reduce the transmission of other respiratory viruses.
The SRV is associated with approximately 30%–40% of all LRTI episodes and seasonal flu epidemics reported that affect 10%–20% of the population each year (20%–40% are children).1,5 During the 2020–2021 season in our cohort neither SRV nor influenza were detected. This finding is seen in the rest of Spain and other countries.3,6,7 The Influenza and other Respiratory Viruses Surveillance System in Spain reported only 6 cases of SRV in the week of 6/2021 from 3732 samples analyzed (0.16%) and 7 cases of influenza since the beginning of the 2020–2021 season. The flu vaccine campaign advanced to October 2020 may have contributed to the decrease in the transmission of the influenza virus. Although detection tests are being performed on an ongoing basis, the rate of respiratory viruses different than SARS-CoV-2 during the 2020–2021 epidemic season remains very low.5
The low rate of respiratory viruses, especially SRV, explains the absence of bronchiolitis during the 2020–2021 autumn–winter season in our cohort, which justifies the heavier weight and older age of patients compared to the pre-pandemic period. These findings are consistent with the data published in the Southern hemisphere during their bronchiolitis epidemic months (April–June).3,8,9 In Australia, the median of hospital admissions due to bronchiolitis in 2020 was 85.9% less than expected, with an 89.1% reduction of PICU admissions.8 In the study conducted by the Collaborative Pediatric Network of Latin America, a 83% reduction of PICU admissions due to LRTI was reported between January 2020 and August 2020 compared to the years 2018–2019.3
During the COVID-19 pandemic, the only viruses detected in our cohort were metapneumovirus (March 2020) and entero/rhinovirus (autumn–winter 2020–2021). It is not clear why—unlike other viruses—the entero/rhinovirus has become so persistent during the pandemic. Britton et al. suggest that in these viruses the absence of a viral envelop makes them less susceptible to inactivation through hand sanitation, therefore making its transmission easier by contact.8
Only 1 case of an ARF admission due to SARS-CoV-2 was reported. It is well known that in the pediatric age, the rate of PICU admission due to SARS-CoV-2 is lower compared to that of other infectious agents and other age groups, which is consistent with the low frequency of COVID-19-related pneumonia seen in our study.
This is the first study published in Spain to report on the low rate of ARF admissions to the PICU setting during the COVID-19 pandemic. More multicenter studies need to be conducted to better analyze the epidemiology of respiratory viruses during the pandemic so that action guidelines can be designed to control the epidemic peaks of the main respiratory viruses in the years to come while taking into consideration the impact that the measures implemented during the pandemic have had reducing the rate of LRTI.
Conflicts of interestNone whatsoever.
Please cite this article as: Bermúdez Barrezueta L, Brezmes Raposo M, Sanz Fernández I, López Casillas P, Villa Francisco C, Pino Vázquez A. Impacto de la pandemia COVID-19 sobre la tasa de ingresos por infecciones respiratorias en Unidad de Cuidados Intensivos Pediátricos. Med Intensiva. 2022;46:281–285.

