

The “National Coordinating Council for Medication Error Reporting and Prevention” (https://www.nccmerp.org/about-medication-errors [updated 16 November 2022]) defines medication error as any avoidable incident that may cause harm to the patient or give rise to inappropriate use of medications, when these are under the control of healthcare professionals, or the patient or consumer.
Intensive Care Units (ICUs) are particularly vulnerable to medication error, due to the many drugs administered to the patients (especially high-risk drugs), and which are mostly given intravenously, with the need for calculating infusion rates. Furthermore, patients admitted to the ICU often present associated organ failure (particularly liver and kidney failure) and/or pharmacokinetic and pharmacodynamic alterations due to the seriousness of the background disease condition. Likewise, most of these patients are sedated, which prevents them from cooperating in the detection and/or prevention of such problems.1
To date, only three studies have described medication errors in the ICU setting in Spain.2–4 We thus decided to carry out a retrospective study of the medication errors in patients admitted to the ICU reported through the CISEMadrid system (see Supplementary material) during 37 months in an 18-bed adult medical-surgical ICU pertaining to a level 2 hospital in Spain. The drug involved, the type of medication error, the impact upon the patient, and the care shift in which the error occurred were recorded. The hospital Research Ethics Committee approved the study on 30 May 2023 (internal code OE 41/2023).
A total of 276 medication errors in the ICU were recorded. Of these, 6 had occurred before patient admission to the ICU and were therefore not included in the study; one was actually not an error; and in 23 cases two types of error were reported. Thus, a total of 294 errors were finally included in the analysis.
Prescription error (63.6%) was the most frequent type of error, followed by administration error (27.5%) (Table 1). These figures are consistent with those published by other authors.2,3,5–7 In hospitals lacking an electronic prescription program, transcription error is the most frequent kind of error.7
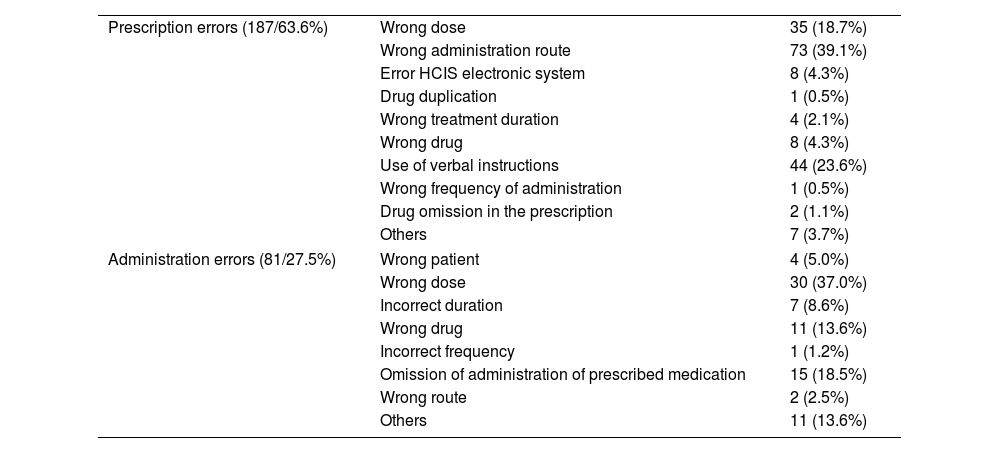
Reported prescription and administration errors.
| Prescription errors (187/63.6%) | Wrong dose | 35 (18.7%) |
| Wrong administration route | 73 (39.1%) | |
| Error HCIS electronic system | 8 (4.3%) | |
| Drug duplication | 1 (0.5%) | |
| Wrong treatment duration | 4 (2.1%) | |
| Wrong drug | 8 (4.3%) | |
| Use of verbal instructions | 44 (23.6%) | |
| Wrong frequency of administration | 1 (0.5%) | |
| Drug omission in the prescription | 2 (1.1%) | |
| Others | 7 (3.7%) | |
| Administration errors (81/27.5%) | Wrong patient | 4 (5.0%) |
| Wrong dose | 30 (37.0%) | |
| Incorrect duration | 7 (8.6%) | |
| Wrong drug | 11 (13.6%) | |
| Incorrect frequency | 1 (1.2%) | |
| Omission of administration of prescribed medication | 15 (18.5%) | |
| Wrong route | 2 (2.5%) | |
| Others | 11 (13.6%) | |
In contrast to those authors who found the most frequent prescription error to be related to the lack of a written full prescription order,3,4,7 dosing error6 or drug omission,9 we found a wrong administration route (39.1%) to be the most common prescription error (e.g., oral route prescribed in a patient subjected to orotracheal intubation). This is probably explained by the use of an electronic prescription program not specific to the ICU that does not allow prescription if all the prescription fields have not been duly completed, but with predefined prescriptions for the entire hospital that were not reviewed or adjusted to the critically ill patient.
Errors related to the use of verbal instructions (23.6%) were a consequence of poorly defined or confusing prescriptions or failure to subsequently prescribe the verbal instruction as indicated in the verbal instructions protocol of our hospital.
As in previous studies,6,7 we found that the most common administration errors were related to the administration of wrong drug doses (37.0%), followed by errors related to the omission of administration of prescribed drugs (18.5%) (Table 1). Most of these problems were related to a lack of training in the use of the electronic prescription system of the hospital.
A recent systematic review10 analyzing prescription errors concerning electronic prescription programs has reported a median error rate of 26.1%, attributable particularly to drug selection and dosing error. The study postulated that although initial data found such programs to apparently improve patient safety in relation to prescription errors, they could generate new errors due to a lack of training in their use, their complexity, system failures, etc. In this context, medication errors attributable to electronic prescriptions need to be separated and analyzed as errors due to the program and errors occurring despite the program.
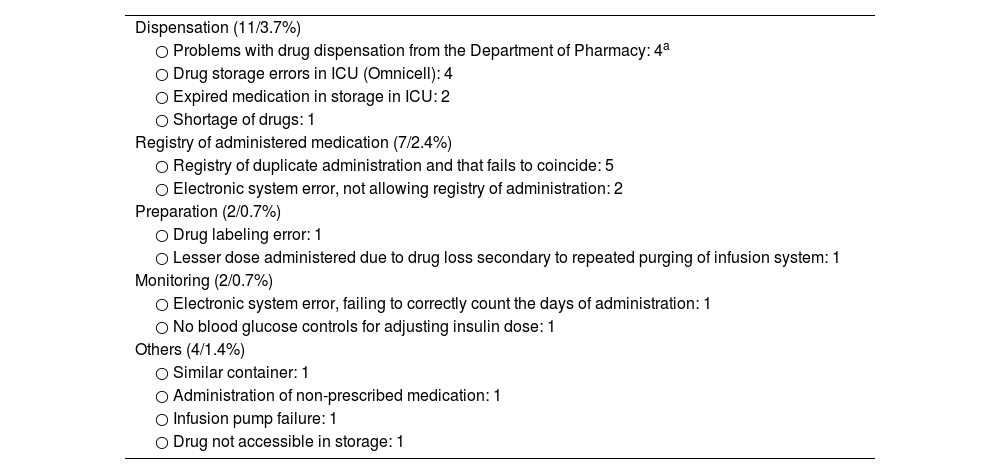
Table 2 describes the rest of the reported errors.
Other reported errors.
| Dispensation (11/3.7%) |
| ○ Problems with drug dispensation from the Department of Pharmacy: 4a |
| ○ Drug storage errors in ICU (Omnicell): 4 |
| ○ Expired medication in storage in ICU: 2 |
| ○ Shortage of drugs: 1 |
| Registry of administered medication (7/2.4%) |
| ○ Registry of duplicate administration and that fails to coincide: 5 |
| ○ Electronic system error, not allowing registry of administration: 2 |
| Preparation (2/0.7%) |
| ○ Drug labeling error: 1 |
| ○ Lesser dose administered due to drug loss secondary to repeated purging of infusion system: 1 |
| Monitoring (2/0.7%) |
| ○ Electronic system error, failing to correctly count the days of administration: 1 |
| ○ No blood glucose controls for adjusting insulin dose: 1 |
| Others (4/1.4%) |
| ○ Similar container: 1 |
| ○ Administration of non-prescribed medication: 1 |
| ○ Infusion pump failure: 1 |
| ○ Drug not accessible in storage: 1 |
The most frequently implicated drugs were fluid therapy and electrolytes (12.6%), antimicrobials (12.2%), sedatives (11.5%) and insulin (7.5%) (Table 1, Supplementary material). In other studies, the most commonly implicated drugs were antibiotics,4,7–10 opiates5 or cardiovascular drugs.9
In 108 cases (36.7%) these problems involved high-risk medications for hospitals according to the Institute for the Safe Use of Medicines (https://www.ismp-espana.org/ficheros/Medicamentos%20alto%20riesgo%20-ISMP.pdf).
Most of the reported errors (79.6%) had no impact on the patient, which is consistent with the findings of other studies, with harmless incidents rates of between 100% and 68.5% of the reported incidents.2,4,5,7
Most of the errors were seen to occur in the course of the morning care shift (43.2%), followed by the night/duty shift (22.4%). Although most prescriptions are made in the morning, there is no work overload or tiredness associated with duty service.
Among the limitations of our study, mention must be made of the fact that we only analyzed the medication errors reported through the CISEMadrid system. As a result, not all actual errors may have been reported, since underreporting is a problem associated with reporting systems. This is due to the existence of many causes or barriers (such as increased workload, concerns about loss of reputation or possible litigation, lack of knowledge, no perception of benefit or fear of disciplinary measures, among others).11 On the other hand, we do not know the prevalence figures, since we did not measure the number of prescriptions made. In turn, as this is a study involving a single center with certain characteristics and a specific electronic prescription program, the conclusions drawn might not be extendable to other hospitals. In contrast, as a strength of our study, and in contrast to previous research, the analyzed reported errors include all the types of error.
In conclusion, medication errors are seen to be common in our ICU. The predominant errors are prescription errors, which in principle are the easiest problems to correct. Most errors do not reach or have an impact on the patient, though due caution is nevertheless required to improve patient safety.
Authors contributionsAll the authors have contributed substantially to the study conception and design; data acquisition, analysis and interpretation; drafting of the manuscript; and have approved the submitted final version.
Financial supportThe present study has received no financial support.
Conflicts of interestThe authors declare that they have no conflicts of interest in relation to the present study.
Thanks are due to all the people involved in patient safety and who have reported the medication errors analyzed in the present study.
The following is Supplementary data to this article:

