

Pharmaconutrients are substrates which in addition to their intrinsic nutritional properties also stimulate immune-favoring mediators, inhibit proinflammatory factors and attenuate the response to injury or aggression. Pharmaconutrients include certain amino acids such as glutamine and arginine, ?-3 fatty acids and some oligoelements and vitamins. At present, due to its effects upon the intestinal barrier and microbiome, dietary fiber is also considered to be a pharmaconutrient.
Since the first description 30 years ago of diets enriched with pharmaconutrients and their clinical application, important controversy has persisted as to the potential usefulness of diets of this kind in the critically ill.
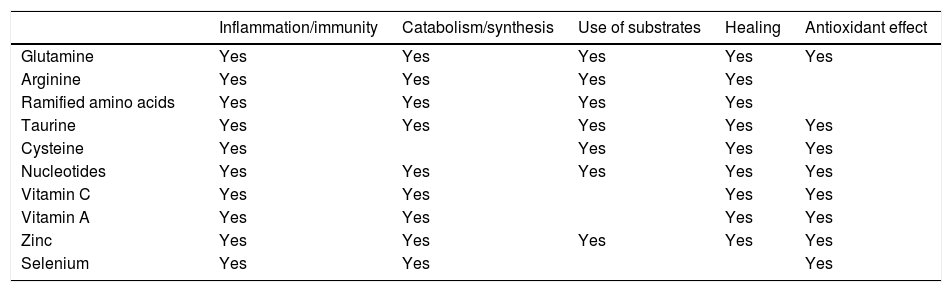
QuestionsDoes the supply of pharmaconutrients and other specific nutrients improve the inflammatory response to injury in the critically ill?Different studies have evidenced that pharmaconutrients can modulate the inflammatory and immune response, modify catabolism, protein synthesis and the use of substrates, and exert a positive influence upon the healing mechanisms. The existing evidence is mainly referred to basic research, though data from clinical studies are also available.1,2 The effects are summarized in Table 1.
Effects of different pharmaconutrients upon metabolic response, inflammation, immune response and healing in situations of injury or aggression.
| Inflammation/immunity | Catabolism/synthesis | Use of substrates | Healing | Antioxidant effect | |
|---|---|---|---|---|---|
| Glutamine | Yes | Yes | Yes | Yes | Yes |
| Arginine | Yes | Yes | Yes | Yes | |
| Ramified amino acids | Yes | Yes | Yes | Yes | |
| Taurine | Yes | Yes | Yes | Yes | Yes |
| Cysteine | Yes | Yes | Yes | Yes | |
| Nucleotides | Yes | Yes | Yes | Yes | Yes |
| Vitamin C | Yes | Yes | Yes | Yes | |
| Vitamin A | Yes | Yes | Yes | Yes | |
| Zinc | Yes | Yes | Yes | Yes | Yes |
| Selenium | Yes | Yes | Yes |
There are a number of enteral nutrition solutions enriched with mixtures of nutrients with the aim of modulating the inflammatory/immune response in the critically ill. The most commonly used mixtures are those containing ?-3 fatty acids (eicosapentaenoic acid [EPA], docosahexaenoic acid [DHA]), gamma-linolenic acid [GLA]) and antioxidants, and those enriched with arginine, ?-3 fatty acids, nucleotides and antioxidants.
A series of meta-analyses have been published on the effects of diets enriched with pharmaconutrients (arginine, ?-3 fatty acids, antioxidants) in the critically ill. All report a decrease in infectious complications, and some of them also evidence a decrease in the duration of hospital stay and of mechanical ventilation.3,4 However, the meta-analyses are characterized by heterogeneity in the composition of the diets employed and in the patient populations included in the studies. Interpretation of the meta-analyses is also a source of controversy.5
Diets enriched with ?-3 fatty acids, GLA and antioxidants have been studied in patients with respiratory failure and in subjects with sepsis. In acute respiratory distress syndrome, such diets can reduce mortality and the duration of mechanical ventilation.6,7 In sepsis, the use of diets of this kind has been associated to a decrease in patient mortality and in progression towards multiorgan failure.7,8
The impact of pharmaconutrition in surgical patients appear to be different, particularly when surgery is elective.9 A meta-analysis of patients following gastrointestinal surgery has shown pharmaconutrition via the enteral route to be superior to other types of nutrition, since it reduces infectious complications, anastomotic leakage and patient mortality.10
Good results have been recorded in severe trauma patients (modulation of the inflammatory response, reduction of infection and improved healing) with the use of diets enriched with pharmaconutrients.11,12
Do critical patients benefit from the administration of glutamine?In quantitative terms, glutamine is the most important amino acid in the body. It represents 50% of the pool of amino acids circulating in plasma. Furthermore, glutamine has important physiological functions referred to tissue protection, antiinflammatory action, immune regulation, the preservation of tissue metabolic functions in situations of stress, and antioxidant action.13 The decrease in glutamine levels seen in situations of stress may be accompanied by deleterious effects such as lessened antioxidant capacity, impaired cell defense mechanisms, diminished intestinal barrier function or increased muscle protein catabolism.14 The augmented use of glutamine in situations of metabolic stress is not compensated by the increase in endogenous synthesis of this amino acid; glutamine is therefore considered to be a semi-essential amino acid in the critically ill.
The supply of large amounts of glutamine during nutritional therapy has been investigated in different groups of critical patients.
The results of the studies that investigate glutamine supply via the enteral route have been contradictory. Overall, the only observed outcome has been a decrease in the duration of hospital stay.15 Nevertheless, in severe burn patients, glutamine supply is associated to a decrease in mortality.15
In contrast, studies that have used glutamine as part of nutritional therapy via the parenteral route have largely evidenced benefits for the patients,16–18 such as fewer infectious complications, a shorter hospital stay and decreased in-hospital mortality. Some studies have reported no positive results or even negative results with the administration of glutamine.19 The REDOX study20 found glutamine administration to be accompanied by deleterious effects when high doses are used, independently of the nutritional regimen involved, and in extremely ill patients (shock with multiorgan failure). The patients investigated in the latter study did not correspond to the group of individuals in which glutamine use is considered in routine clinical practice, however.
It should be noted that the studies that have investigated the effects of parenteral glutamine are heterogeneous both in design and in the form of glutamine used (free glutamine or glutamine dipeptides). On analyzing the studies that have used alanine-glutamine dipeptides as part of the nutritional regimen, a favorable effect is seen in terms of infectious complication, hospital stay or mortality.21
Is there evidence supporting the use of pharmaconutrients dissociated from the administration of specialized nutritional therapy?Some authors have investigated the strategy of supplying pharmaconutrients independently and dissociated from nutritional therapy with the purpose of covering the nutritional objectives (dissociated pharmaconutrition). This allows the administration of “therapeutic” doses of pharmaconutrients without awaiting patient tolerance of all the enteral nutrition. However, this strategy generates controversy regarding the timing of pharmaconutrient supply, the indicated administration route, and whether such dissociated pharmaconutrition offers advantages for the patients.
The administration of glutamine supplements via the enteral route, independently of nutritional therapy, can reduce the duration of multiorgan dysfunction,22 though other studies have evidenced that this strategy does not result in beneficial effects for the patient.23 When using the parenteral route, dissociated glutamine supplementing likewise does not afford beneficial effects.24 The enteral and parenteral supply of high doses of glutamine in patients under conditions of shock and multiorgan dysfunction has been found to have harmful effects (increased mortality).20
The dissociated provision of ?-3 fatty acids via both the enteral25 and the parenteral route26 has yielded contradictory results in terms of the inflammatory reaction markers. This treatment strategy is not accompanied by beneficial clinical effects for the patients. In contrast, it may be associated to a prolongation of mechanical ventilation, organ dysfunction, and a longer stay in intensive care.25
Should all critical patients with enteral nutrition receive fiber? What type of fiber is indicated?Diet fibers are plant oligosaccharides or polysaccharides that cannot by hydrolyzed by the endogenous small bowel enzymes of humans. There are two types of fiber: insoluble and soluble. The main effect of insoluble fiber is mechanical (conformation of the fecal bolus). The main risk associated to this type of fiber is intestinal obstruction and ischemia, given the motility problems of the critically ill.
Soluble (fermentable) fiber in turn gives rise to short chain fatty acids (SCFAs) thanks to the action of the intestinal microbiota. Short chain fatty acids constitute a source of energy for the colon mucosal cells and exert effects upon colon epithelial cell proliferation and differentiation, with an increase in blood flow, a decrease in colon pH, the stimulation of pancreatic secretion, increased water and sodium absorption, and the regulation of intestinal motility and of the microbiota.
The use of the different types of fiber and the amounts to be supplied have been the subject of many studies and meta-analyses, though few firm conclusions have been drawn, due to the heterogeneity of the studies, formulas used and doses administered.27 In general, soluble fiber appears to reduce the frequency of diarrhea associated to enteral nutrition.28
Do the critically ill benefit from the administration of probiotics or a mixture of prebiotics and probiotics (synbiotics)?The intestinal flora has important functions in terms of protection against infection, drug metabolism, vitamin synthesis and the response to disease. In the critically ill, many circumstances lead to loss of the normal intestinal microbiota and to the intraluminal overgrowth of pathogens (dysbiosis).29 The consequences of this are catastrophic, for in addition to loss of the capacity to maintain barrier functions, alteration of the microbiota in the critically ill is associated to an increased production of cytokines, cell apoptosis and immunosuppression, and all this leads to bacterial translocation into the systemic and lymphatic circulation, nosocomial infection and, ultimately, multiorgan dysfunction.
The use of probiotics (defined by the World Health Organization [WHO] as non-pathogenic live microorganisms which when supplied in adequate amounts afford health benefits) and of prebiotics (fermentable fiber) seeks to restore the balance between beneficial and pathogenic bacteria. Synbiotics are formulations containing both probiotics and prebiotics, favoring survival of the administered strains and, in sum, restoration of the intestinal flora.
The published meta-analyses of studies that have investigated the consequences of administering probiotics and synbiotics in the critically ill describe a decrease in infectious complications30 and a positive effect in terms of the prevention of ventilator-associated pneumonia.31
However, the use of probiotics in the critically ill is not without risks particularly in the form of intestinal ischemia and the development of fungal infections – though these are infrequent.
Recommendations- •
The use of pharmaconutrients could be considered as a therapeutic strategy seeking to modulate the inflammatory/immune response in the critically ill (Level of evidence: low. Degree of recommendation: low).
- •
The use of enteral diets enriched with mixtures of pharmaconutrients (arginine, ?-3 fatty acids, antioxidants) is suggested in postsurgery critically ill patients and in cases of severe trauma (Level of evidence: moderate. Degree of recommendation: moderate).
- •
The use of enteral diets enriched with ?-3 fatty acids, docosahexaenoic acid (DHA) and antioxidants could be considered in patients with sepsis (Level of evidence: low. Degree of recommendation: low).
- •
Glutamine dipeptide at adequate doses (0.25–0.35?g of glutamine/kg b.w./day), in the absence of contraindications, is suggested as part of nutritional therapy in the critically ill receiving parenteral nutrition (Level of evidence: moderate. Degree of recommendation: moderate).
- •
Glutamine supplementing via the enteral route is suggested in burn patients (Level of evidence: moderate. Degree of recommendation: moderate).
- •
The supply of pharmaconutrients dissociated from the nutritional regimen is not routine practice and is not suggested in the critically ill (Level of evidence: moderate. Degree of recommendation: moderate).
- •
The use of diets containing 100% insoluble fiber in the critically ill is not recommended (Level of evidence: low. Degree of recommendation: high).
- •
The routine use of diets containing fiber mixtures (insoluble/fermentable) for the prevention of diarrhea associated to enteral nutrition is not advised (Level of evidence: expert opinion. Degree of recommendation: low).
- •
Diets with a high soluble fiber content are advised among the measures for controlling diarrhea associated to enteral nutrition (Level of evidence: expert opinion. Degree of recommendation: moderate).
- •
The routine use of probiotics in critically ill patients receiving enteral nutrition is not advised (Level of evidence: low. Degree of recommendation: moderate).
Dr. Montejo-González has received payment for participation in activities financed by B. Braun, Vegenat Nutrición, Nestlé Healthcare Nutrition, Abbott Nutrition, Baxter and Nutricia in the form of conferences, counseling, the organization of scientific congresses, courses, scientific meetings, and for participation in congresses and scientific meetings. Dr. de la Fuente O’Connor declares that she has no conflicts of interest. Dr. Martínez-Lozano has received funding from Nestlé and Nutricia for participation in scientific congresses, and from Vegenat for participation in scientific meetings. Dr. Serviá-Goixart has received payment from Fresenius Kabi and Abbott for participation in congresses and scientific meetings.
Note to supplementThis article forms part of the supplement “Recommendations for specialized nutritional-metabolic management of the critical patient. Metabolism and Nutrition Working Group of the Spanish Society of Intensive and Critical Care Medicine and Coronary Units (SEMICYUC)”, with the sponsorship of Abbott Nutrition.
Please cite this article as: Montejo González JC, de la Fuente O’Connor E, Martínez-Lozano Aranaga F, Servià Goixart L. Recomendaciones para el tratamiento nutrometabólico especializado del paciente crítico: farmaconutrientes, nutrientes específicos, fibra, simbióticos. Grupo de Trabajo de Metabolismo y Nutrición de la Sociedad Española de Medicina Intensiva, Crítica y Unidades Coronarias (SEMICYUC). Med Intensiva. 2020;44:39–43.

