

Several studies1–3 have concluded that patients requiring invasive ventilatory support due to acute respiratory distress syndrome (ARDS) associated with coronavirus disease 2019 (COVID-19) present a course and prognosis different from those seen in other disease conditions.
However, few studies4,5 have specifically analyzed the mechanical ventilation (MV) weaning process in COVID-19.
The present scientific letter describes the characteristics of this weaning process in a population of patients with ARDS secondary to COVID-19 in our setting, and analyzes the clinical outcomes according to the WIND (Weaning according to a New Definition)6 and ICC (International Consensus Conference) classifications.7
A post hoc analysis was performed of patients enrolled in a prospective clinical trial from March to September 2021. The study, which adhered to the CONSORT criteria,8 was registered in ClinicalTrials.gov (NCT05012267). Patients over 18 years of age that met the following criteria were included: ARDS secondary to COVID-19 defined according to the Berlin specifications9 and with an indication for prone positioning based on the criteria of the PROSEVA trial.10 The patients were randomized to a prolonged (48 h) or short-prone position strategy (>16 h). A retrospective observational study of the aspects related to the weaning process was subsequently carried out.
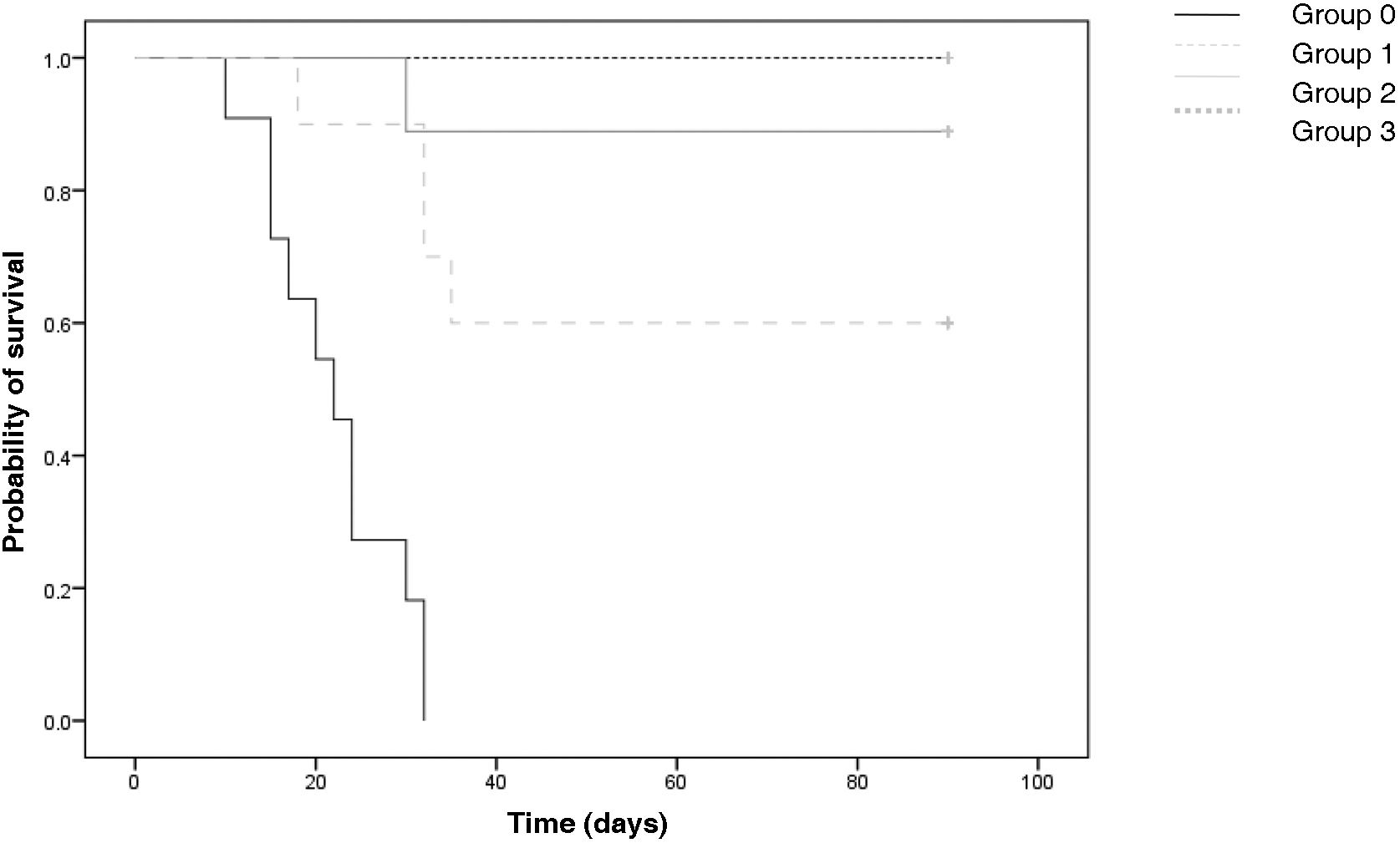
Continuous variables were reported as the mean and standard deviation (SD) or as the median and interquartile range (IQR), while categorical variables were reported as frequencies and percentages. Normal data distribution was analyzed using the Kolmogorov-Smirnov test, and the differences between the weaning groups were analyzed with the Student t-test or analysis of variance (ANOVA) for continuous variables and Pearson’s chi-square test or the Kruskal-Wallis test for categorical variables. The survival analysis considered mortality as the primary endpoint. The Kaplan-Meier method was used to plot the survival curves, and the log-rank test was applied for comparison of the curves.
Statistical significance was considered for p ≤ 0.05. The SPSS version 25.0 statistical package (IBM Corp., Armonk, NY, USA) was used throughout.
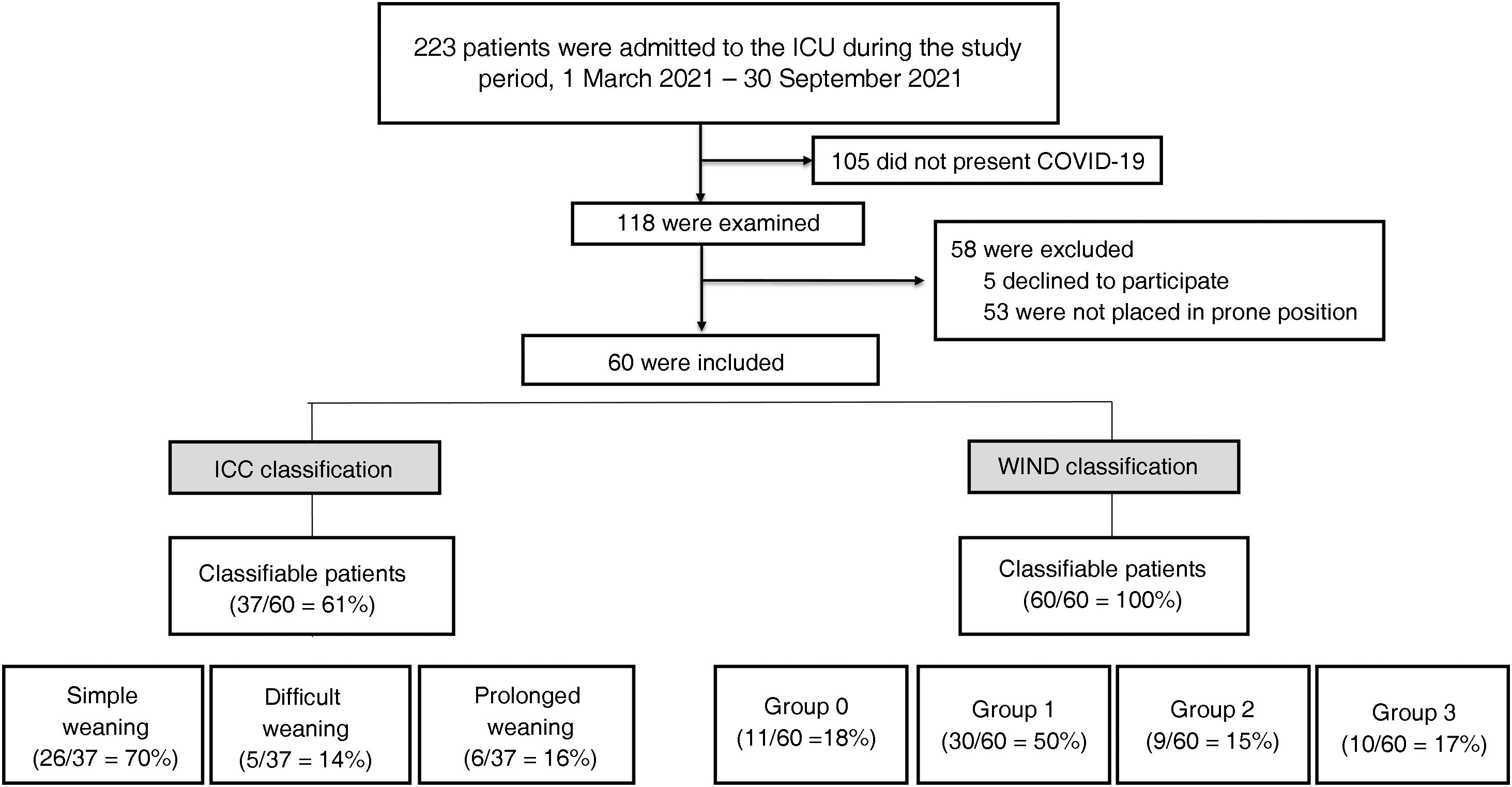
During the study period, 223 patients were admitted to the Intensive Care Unit (ICU), and of these, 118 presented COVID-19 (Fig. 1). A total of 60 patients were included in the study.

All patients were classified according to the WIND criteria as follows: group 0, n = 11 (18%), group 1, n = 30 (50%), group 2, n = 9 (15%) and group 3, n = 10 (17%). Only 37 patients (62%) could be classified according to the ICC criteria (Supplementary Tables 1 and 2): simple weaning, n = 26 patients (70%), difficult weaning, n = 5 patients (14%), and prolonged weaning, n = 6 (16%). The baseline characteristics and initial ventilatory parameters of the global population and of the different WIND groups, as well as the clinical outcomes, are reported in Supplementary Table 3. The concordance analysis of the results between the two classifications is described in Supplementary Table 1. Of the 23 patients not classifiable according to the ICC criteria, 11 (47%) were included in group 0, as no MV weaning attempt was made. In contrast, the remaining 12 (52%) were included in group 1 (n = 4), group 2 (n = 4) and group 3 (n = 4). In these cases, classification according to the ICC criteria was not possible due to death occurring before extubation (n = 5) or tracheotomy performed before starting the weaning process (n = 7).
During the study period, 49 patients (82%) experienced some MV weaning attempt. The first attempt was a spontaneous breathing trial in 35 patients (71%), direct extubation in four (9%), and a spontaneous breathing trial over tracheotomy in 10 (20%). The first weaning attempt proved successful in 35/49 cases (71%).
Among all the included patients, successful weaning occurred in 37 cases (62%), while reintubation during admission to the ICU was recorded in 8 (21%). The mean time to reintubation was one day. The patients requiring reintubation presented a mortality rate of 25%, versus 0% among the patients not requiring reintubation.
Tracheotomy was performed in 22 patients (37%), with a median time from orotracheal intubation to tracheotomy of 11 days (range 8–14). Of the patients subjected to tracheotomy, 9 died (41%), while the rest could be successfully weaned.
On examining the clinical outcomes, both classifications showed increased complexity of the weaning process to be associated with longer ICU and hospital stays, and longer times under sedation and neuromuscular block. However, a correlation to mortality was only observed in the case of the WIND classification (Fig. 2 and Supplementary Tables 3 and 4).
.")
This secondary analysis of patients with ARDS as a consequence of COVID-19 offers epidemiological information on the invasive MV weaning process not previously analyzed in our setting. The main findings can be summarized as follows: 1) Almost 20% of the patients did not experience a first MV weaning attempt; 2) Sixty-two percent of the patients were extubated, and one out of every 5 required reintubation; 3) Tracheotomy was performed in 37% of the cases; 4) The ICC classification was unable to analyze almost 40% of the patients, with no differences in mortality between its groups; 5) The WIND classification was able to analyze all the patients in the sample, stratifying them into groups characterized by a gradual increase in morbidity and mortality.
The present study has several limitations, including its single-center design and small sample size. Although the fact that the study was carried out in a single center limits the heterogeneity of the weaning process, the latter was not carried out following a strict protocol. Lastly, given the objectives of the study, no search was made for independent factors associated with the clinical outcomes.
Financial supportThe present study has received no financial support.
Statement on generative AI and AI assisted technologies in the drafting processNo artificial intelligence tool was used in the preparation of this work.
Conflicts of interestThe authors declare that they have no conflicts of interest.
We wish to thank the staff of the Department of Intensive Care Medicine of Hospital Universitario 12 de Octubre (physicians, nurses auxiliary staff, physiotherapists and others) for their admirable work and dedication during the COVID-19 pandemic.
The following is Supplementary data to this article:

