


Liver transplantation (LT) is characterized by bleeding, circulatory volume fluctuations, vascular clamping/unclamping and major fluid shifts, resulting in significant circulatory instability.1 A meta-analysis conducted by Cecconi et al. concluded that hemodynamic monitoring strategies coupled with therapy decisions, reduces mortality in high-risk surgical patients.2 Invasive thermodilution has long been the gold standard in estimating cardiac output (CO).3 As an easy-to-use noninvasive device, NICOM® uses thoracic bioreactance to analyze the variations in voltage in each cardiac contraction in response to high-frequency current. Previous studies have shown mixed results regarding the performance of bioreactance for measuring CO in various populations.4-6 We aimed to evaluate whether bioreactance can be used as an alternative CO monitoring technique in liver transplantation.
We performed a prospective non-randomized study from September to November 2019 and recruited all patients admitted for elective LT. Re-transplants or emergency LT were excluded. All patients had a Pulse Contour Cardiac Output (PiCCO®) device placed in the femoral artery and a central venous catheter placed in the internal jugular vein according to the established transplant's protocol. After LT surgery, patients were sequentially included for placing a Cheetah Medical NICOM® device. Cardiac index (CI) was recorded at admission and every 8h during the first 48h. CI recorded from PiCCO® was measured three times using the transpulmonary thermodilution technique and after injecting 20mL boluses of cold normal saline via a central venous catheter. System was calibrated before each group of measurements and performed by the same person. If the variation among readings was higher than 10%, one additional measurement was taken for an average reading. Data was expressed as mean values and standard deviation (SD). The difference in CO between the two techniques was calculated as the mean±1.96×SD which were called 95% limits of agreement; the percentage error was calculated using the formula (100×1.96×SD of bias between the two methods)/mean between the two methods. Mean percentage error was considered acceptable if <30%. Correlations were tested using the Pearson correlation coefficient. Agreement between thermodilution/bioreactance was tested using Bland–Altman analysis and intraclass correlation coefficient (ICC).5-7 Conclusions obtained from bioreactance did not influence medical decisions. Institution Ethics Committee approved the study.
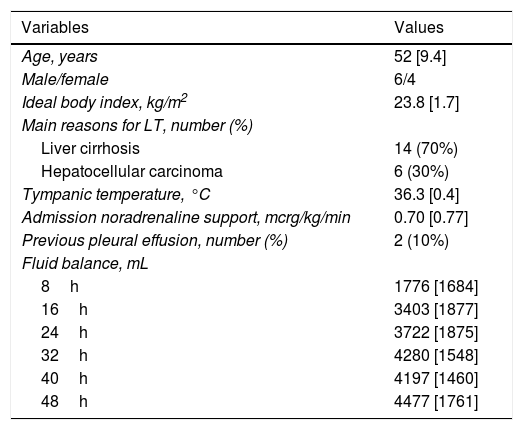
Twenty-nine patients were recruited but only 20 fulfilled the inclusion criteria. A total of 420 paired observations were collected as described in Table 1. After LT, as a result of fluid resuscitation, cumulative fluid balance increased as well as ELWI measurements. There was good agreement between thermodilution-CI and bioreactance-CI (3.44±0.87 versus 3.51±0.738, L/min/m2) at ICU admission, with a mean bias of −0.076L/min/m2 and an ICC of 0.974 (95% confidence interval 0.932–0.990, P<0.05). The mean percentage error between the two methods was ±14%. There was a strong correlation between thermodilution-CI and bioreactance-CI (Table 1 and Fig. 1). Over time, CI measurements were progressively different in both devices and mean percentage error was >30% (Table 1).
Postoperative clinical data after liver transplant.
| Variables | Values |
|---|---|
| Age, years | 52 [9.4] |
| Male/female | 6/4 |
| Ideal body index, kg/m2 | 23.8 [1.7] |
| Main reasons for LT, number (%) | |
| Liver cirrhosis | 14 (70%) |
| Hepatocellular carcinoma | 6 (30%) |
| Tympanic temperature, °C | 36.3 [0.4] |
| Admission noradrenaline support, mcrg/kg/min | 0.70 [0.77] |
| Previous pleural effusion, number (%) | 2 (10%) |
| Fluid balance, mL | |
| 8h | 1776 [1684] |
| 16h | 3403 [1877] |
| 24h | 3722 [1875] |
| 32h | 4280 [1548] |
| 40h | 4197 [1460] |
| 48h | 4477 [1761] |
| Variables | Thermodilution | NICOM | P-value |
|---|---|---|---|
| Cardiac index, L/min/m2 | |||
| 0h | 3.44 [0.870] | 3.51 [0.738] | 0.494 |
| 8h | 3.77 [0.827] | 3.42 [0.483] | 0.124 |
| 16h | 3.85 [1.21] | 3.65 [1.04] | 0.195 |
| 24h | 3.77 [0.731] | 3.38 [0.856] | 0.255 |
| 32h | 3.86 [0.509] | 3.21 [1.25] | 0.078 |
| 40h | 3.85 [0.545] | 3.25 [1.17] | 0.109 |
| 48h | 3.87 [0.449] | 3.2 [1.17] | 0.080 |
| ELWI, mL/kg | |||
| 0h | 7.73 [1.79] | – | – |
| 8h | 8.50 [1.86] | ||
| 16h | 8.81 [2.08] | ||
| 24h | 9.21 [1.88] | ||
| 32h | 9.5 [1.90] | ||
| 40h | 9.5 [1.65] | ||
| 48h | 8.9 [1.21] | ||
| CI agreement | 0h | 24h | 48h |
|---|---|---|---|
| Bias and limits of agreement | −0.076 (−0.199 to 0.047) | 0.411 (−1.843 to 2.67) | 0.560 (−1.914 to 3.034 |
| ICC (95% confidence interval) | 0.974 (0.932 to 0.990) | −0.115 (−1.983 to 0.611) | −0.630 (−3.396 to 0.470) |
| Correlation (r, P-value) | 0.167, P<0.05 | −0.276, P=0.644 | −1.522, P<0.05 |
| Mean percentage error | ±14% | ±61% | ±69% |
CI: cardiac index; ELWI: extra lung water index; ICC: intraclass correlation coefficient; LT: liver transplant.
Continuous variables were presented as mean and standard deviation (SD). Independent data was compared using Student's unpaired t-test. Correlations were tested using the Pearson correlation coefficient. We calculated the percentage error between CI measurements using the following formula: mean percentage error=(100×1.96×SD of bias between the two methods)/mean between the two methods. Mean percentage error was considered acceptable if <30%.
, after 24h (B) and after 48h (C) of monitoring.")
Non-invasive CI monitoring by the bioreactance technique has gained considerable interest recently. In patients after cardiac surgery, NICOM® had good agreement with thermodilution, the currently accepted gold standard.3,4 Our results suggest that after the first hours, NICOM® was a valid method for assessing CI, when compared with CI measured by invasive thermodilution. The mean percentage error obtained in the first measure was 14%, which is less than the recommended cut-off of 30%. However, over time, we consistently observed percentage errors >50%, which doubts its use. Bioreactance depends on the analysis of the difference in high-frequency current signal that traverses the thoracic cavity, which is influenced by the amount of fluids in the thorax.3 In our population, cumulative fluid balance during the first two days, associated with a high ELWI may have interfered with signal reception and CI calculation. For this reason, we excluded 9 patients with acute phase disturbs (re-transplants or urgent LT) as a way to reduce bias. Furthermore, our study's interpretations were limited by a relatively small sample size and the absence of NICOM® measurements during surgery. Hemoglobin concentration and hematocrit values should be taken into count as they may increase the bias between the two methods.
In sum, our observation showed unacceptable agreement between bioreactance and thermodilution for assessing CI in the postoperative phase of LT. Thus, in this population, bioreactance as a substitute to thermodilution in spite of its noninvasiveness, did not reveal to be an alternative.
FundingNo sources of funding for the present paper were used.
Conflict of interestsThe authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.

