


Analizar qué variables asociadas al ingreso en UCI-COVID se asociaron con pacientes que generaron un mayor coste hospitalario según el APR-GRD.
DiseñoEstudio retrospectivo, observacional y analítico.
ÁmbitoUCI-COVID de hospital terciario.
PacientesMayores de 18 años, con diagnóstico confirmado de enfermedad por SARS-CoV-2.
IntervencionesModelos predictivos mediante regresión logística múltiple.
Variables de interés principalesCoste hospitalario, APR-GRD, ventilación mecánica.
ResultadosSe analizaron 799 pacientes, categorizados por terciles según el coste de su estancia hospitalaria, obteniendo 3 grupos: 266 enfermos con menor coste (mediana de 6.160€ [p25: 3.962-p75: 6.160]); 314 que generaron un coste intermedio (mediana de 16.446€ [p25: 10.653-p75: 18.274]), y 219 con mayor coste hospitalario (mediana de 26.085€ [p25: 26.085-p75: 51.523]). El mejor modelo predictivo, con un AIC de 490,09 y un R2 de 0,32, identificó como factores asociados a un mayor coste hospitalario la estancia en UCI (OR: 1,05; IC95%: 1,03-1,07; p<0,01), el desarrollo de TAVM/NAVM (OR: 4,72; IC95%: 2,83-7,85; p<0,01), la infección por OXA-48 (OR: 2,65; IC95%: 1,25-5,61; p=0,01), el tromboembolismo pulmonar (OR: 6,42; IC95%: 2,17-19,26; p<0,01), el hábito tabáquico (OR: 2,22; IC95%: 1,49-3,74; p<0,01) y la necesidad de vasopresores (OR: 1,79; IC95%: 1,22-2,86; p=0,01). El área bajo la curva obtenida fue de 0,866, con un valor de p<0,01.
ConclusionesLa estancia prolongada en UCI, las complicaciones infecciosas y tromboembólicas, el hábito tabáquico y la necesidad de vasopresores se asociaron significativamente con un mayor coste hospitalario.
To analyse which variables associated with ICU admission for COVID-19 were linked to higher hospital costs according to the APR-DRG classification.
DesignRetrospective, observational, and analytical study.
SettingCOVID-19 ICU in a tertiary hospital.
PatientsAdults (>18 years) with a confirmed diagnosis of SARS-CoV-2 infection.
InterventionsPredictive models using multiple logistic regression.
Main variables of interestHospital cost, APR-DRG, mechanical ventilation.
ResultsA total of 799 patients were analysed and categorized into tertiles based on hospital stay costs, resulting in 3 groups: 266 patients with lower costs (median €6,160 [p25: 3,962-p75: 6,160]), 314 with intermediate costs (median €16,446 [p25: 10,653-p75: 18,274]), and 219 with higher costs (median €26,085 [p25: 26,085-p75: 51,523]). The best predictive model, with an AIC of 490.09 and an R2 of 0.32, identified the following factors as significantly associated with higher hospital costs: ICU length of stay (OR: 1.05; 95% CI: 1.03-1.07; p<0.01), development of VAT/VAP (OR: 4.72; 95% CI: 2.83-7.85; p<0.01), OXA-48 infection (OR: 2.65; 95% CI: 1.25-5.61; p=0.01), pulmonary embolism (OR: 6.42; 95% CI: 2.17-19.26; p<0.01), smoking history (OR: 2.22; 95% CI: 1.49-3.74; p<0.01), and vasopressor requirement (OR: 1.79; 95% CI: 1.22-2.86; p=0.01). The area under the curve was 0.866 (p<0.01).
ConclusionsProlonged ICU stay, infectious and thromboembolic complications, smoking history, and vasopressor requirement were significantly associated with higher hospital costs.
Durante la pandemia, la expansión de las camas y la implementación de unidades específicas para pacientes con COVID-19 (UCI-COVID) fueron estrategias que implicaron un aumento extraordinario del gasto sanitario1.
Si bien existen estudios sobre los costes hospitalarios derivados de la pandemia, el conocimiento sobre qué factores específicos dentro del ingreso en UCI-COVID se asocian con un mayor gasto sanitario es escaso. Las investigaciones al respecto muestran resultados de gasto heterogéneos según los recursos disponibles, el método de estudio empleado en el cálculo de gasto y el nivel sociosanitario de la región estudiada1–4.
En este contexto, los Grupos Relacionados por el Diagnóstico (GRD, DRG en su versión inglesa) son un sistema de clasificación de pacientes atendidos en régimen de hospitalización con internamiento, que agrupan los casos atendidos en función de los costes necesarios para su atención, manteniendo una cierta coherencia clínica en los grupos elaborados. All Patient Refined (APR)-GRD introduce 2 nuevos criterios principales en la clasificación: severidad y riesgo de mortalidad5,6. No obstante, algunos autores han cuestionado que este enfoque haga justicia al impacto que diferentes factores y variables derivadas durante el ingreso en un servicio de medicina intensiva (SMI) tienen en los gastos hospitalarios7.
Del mismo modo, hay que tener en cuenta que algunos estudios de coste-beneficio pueden presentar una elevada complejidad metodológica o estar sujetos a sesgos, lo que dificulta su interpretación y aplicación en la práctica clínica. No obstante, es fundamental determinar el impacto de aquellas variables que los profesionales sanitarios identifican en la atención diaria y que, potencialmente, pueden influir en el coste hospitalario. La identificación y cuantificación precisa de estos factores permitiría optimizar la asignación de recursos y mejorar la eficiencia en la gestión asistencial, desde el nivel clínico.
Este trabajo tiene como objetivo analizar qué variables asociadas al ingreso en UCI-COVID –incluyendo factores clínico-demográficos, comorbilidades, estrategias terapéuticas, evolución clínica y complicaciones– se asocian con pacientes que generaron un mayor coste hospitalario según el APR-GRD.
MétodoEstudio retrospectivo de cohortes, llevado a cabo en el SMI de un hospital universitario de tercer nivel de 850 camas, con un área de población asignada cercana a los 300.000 habitantes. Fueron incluidos los enfermos adultos que habían ingresado en UCI-COVID del SMI entre marzo de 2020 y marzo de 2022 con diagnóstico confirmado de infección por SARS-CoV-2 mediante reacción en cadena de la polimerasa en células del tracto respiratorio.
Los datos fueron recopilados en el registro de la cohorte de pacientes con COVID-19 del SMI. Este registro se llevó a cabo tras obtener la aprobación del Comité de Ética en Investigación local (código de referencia local 2020.250) y obtener el consentimiento informado de los pacientes o sus representantes legales –de forma escrita y/o telefónica– para introducir sus datos en el mismo. Posteriormente, algunos datos que no fueron inicialmente recopilados se completaron de manera retrospectiva.
Fueron criterios de inclusión: ser mayor de 18 años, tener un diagnóstico confirmado de enfermedad por SARS-CoV-2 en las primeras 24h de ingreso hospitalario y la necesidad de ingreso en la UCI-COVID. El detalle de las variables registradas se muestra en el material suplementario. Se excluyeron del análisis los pacientes que, al depurar la base de datos, presentaron inconsistencias en las variables o carecían de datos básicos, aquellos que reingresaron en la UCI durante el mismo episodio hospitalario (es decir, con más de un ingreso) y los que fueron trasladados a otros centros por razones ajenas a la decisión médica de alta.
Los APR-GRD, así como el tipo de alta, los diagnósticos y procedimientos codificados al alta hospitalaria, la severidad de la enfermedad por APR-GRD y el riesgo de muerte fueron obtenidos a través del Conjunto Mínimo Básico de Datos de las altas hospitalarias facilitados por el Servicio de Admisión y Documentación Clínica del centro. Los precios públicos por proceso, y su identificación con cada proceso hospitalario mediante su APR-GDR, se obtuvo de la Orden que fija las cuantías de los Precios Públicos de los Servicios Sanitarios prestados por el Servicio Cántabro de Salud8.
Los enfermos fueron categorizados en terciles, según el coste hospitalario derivado del APR-GRD. Se obtuvieron 3 grupos de coste hospitalario: primer grupo de menor coste, segundo grupo de coste intermedio y tercer tercil o grupo de mayor coste hospitalario.
Se realizó el seguimiento de los pacientes durante 90 días desde el momento de ingreso en la UCI hasta el alta hospitalaria o hasta su fallecimiento (hecho que se produjese primero). Los costes de los enfermos fueron considerados hasta el alta hospitalaria o hasta el fallecimiento del mismo durante el ingreso.
Se realizó un análisis descriptivo de la muestra, donde las variables categóricas se presentan como frecuencia absoluta y porcentaje, y como mediana y sus percentiles 25-75 (p25-75) las variables cuantitativas continuas. Las comparaciones de proporciones entre los grupos se realizaron mediante la prueba chi cuadrado. Para la comparación de medias entre grupos se utilizó el ANOVA en las variables que presentaron distribución normal. En las variables que no seguían una distribución normal se utilizó la prueba de Kruskal-Wallis para comparar los grupos. En caso de obtener diferencias significativas, se realizaron comparaciones por pares entre los grupos de terciles de coste hospitalario, aplicando la prueba de Dunn con corrección de Bonferroni para ajustar el error de tipo i debido a múltiples comparaciones. Se utilizó un nivel de significación de α=0,05.
Para evaluar la asociación entre las distintas variables potencialmente pronósticas y el alto coste hospitalario (tercer tercil de coste) se realizó un análisis de regresión logística bivariante. Posteriormente, las variables que alcanzaron significación estadística en dicho análisis fueron incluidas en modelos predictivos mediante regresión logística múltiple. Para la selección del modelo óptimo, se utilizaron los criterios de información de Akaike (AIC) y de Bayes (BIC), con el objetivo de identificar el modelo con mejor capacidad predictiva y ajuste.
Los diagnósticos de multicolinealidad mostraron que todas las variables incluidas en el modelo presentan tolerancias superiores a 0,80 y factores de inflación de la varianza por debajo de 1,3, lo que indica ausencia de colinealidad preocupante.
El análisis de los datos se realizó utilizando JASP versión 0.19.3 (Países Bajos).
ResultadosDurante el periodo analizado ingresaron un total de 911 enfermos en la UCI-COVID. Fueron finalmente analizados 799 pacientes que cumplían los criterios de inclusión (ver diagrama de flujo en la figura 1).

Los 799 pacientes fueron categorizados por terciles según el coste de su estancia hospitalaria, obteniendo 3 grupos: 266 enfermos con menor coste (mediana de 6.160€ [p25: 3.962-p75: 6.160]); 314 que generaron un coste intermedio (mediana de 16.446€ [p25: 10.653-p75: 18.274]), y 219 con mayor coste hospitalario (mediana de 26.085€ [p25: 26.085-p75: 51.523]).
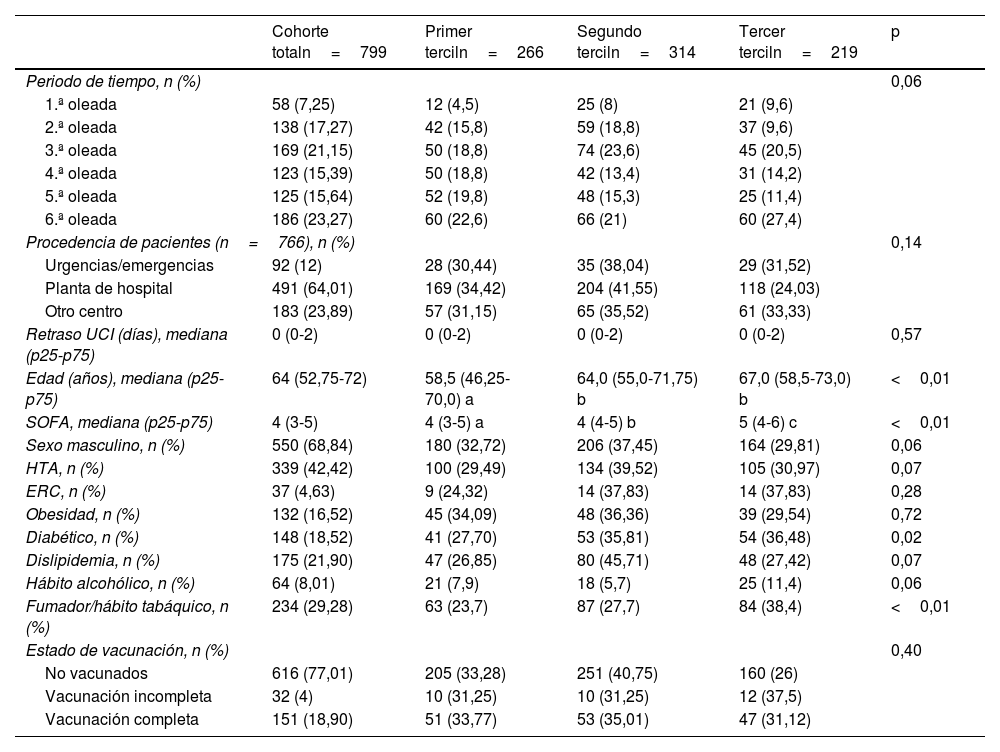
En la cohorte total de 799 pacientes, la distribución a lo largo de las 6 oleadas mostró una mayor incidencia en la sexta oleada (23,27%). La edad mostró diferencias significativas (p<0,01), con una mediana de 58,5 años en el primer tercil y 67 años en el tercero. El Sequential Organ Failure Assessment también aumentó progresivamente entre terciles (p<0,01). Entre comorbilidades, la diabetes (p=0,02) y el hábito tabáquico estuvieron más presentes en el tercer tercil de coste (p<0,01) (tabla 1).
Características demográficas y clínicas de los pacientes de la cohorte analizada y diferencias según el tercil de coste hospitalario
| Cohorte totaln=799 | Primer terciln=266 | Segundo terciln=314 | Tercer terciln=219 | p | |
|---|---|---|---|---|---|
| Periodo de tiempo, n (%) | 0,06 | ||||
| 1.ª oleada | 58 (7,25) | 12 (4,5) | 25 (8) | 21 (9,6) | |
| 2.ª oleada | 138 (17,27) | 42 (15,8) | 59 (18,8) | 37 (9,6) | |
| 3.ª oleada | 169 (21,15) | 50 (18,8) | 74 (23,6) | 45 (20,5) | |
| 4.ª oleada | 123 (15,39) | 50 (18,8) | 42 (13,4) | 31 (14,2) | |
| 5.ª oleada | 125 (15,64) | 52 (19,8) | 48 (15,3) | 25 (11,4) | |
| 6.ª oleada | 186 (23,27) | 60 (22,6) | 66 (21) | 60 (27,4) | |
| Procedencia de pacientes (n=766), n (%) | 0,14 | ||||
| Urgencias/emergencias | 92 (12) | 28 (30,44) | 35 (38,04) | 29 (31,52) | |
| Planta de hospital | 491 (64,01) | 169 (34,42) | 204 (41,55) | 118 (24,03) | |
| Otro centro | 183 (23,89) | 57 (31,15) | 65 (35,52) | 61 (33,33) | |
| Retraso UCI (días), mediana (p25-p75) | 0 (0-2) | 0 (0-2) | 0 (0-2) | 0 (0-2) | 0,57 |
| Edad (años), mediana (p25-p75) | 64 (52,75-72) | 58,5 (46,25-70,0) a | 64,0 (55,0-71,75) b | 67,0 (58,5-73,0) b | <0,01 |
| SOFA, mediana (p25-p75) | 4 (3-5) | 4 (3-5) a | 4 (4-5) b | 5 (4-6) c | <0,01 |
| Sexo masculino, n (%) | 550 (68,84) | 180 (32,72) | 206 (37,45) | 164 (29,81) | 0,06 |
| HTA, n (%) | 339 (42,42) | 100 (29,49) | 134 (39,52) | 105 (30,97) | 0,07 |
| ERC, n (%) | 37 (4,63) | 9 (24,32) | 14 (37,83) | 14 (37,83) | 0,28 |
| Obesidad, n (%) | 132 (16,52) | 45 (34,09) | 48 (36,36) | 39 (29,54) | 0,72 |
| Diabético, n (%) | 148 (18,52) | 41 (27,70) | 53 (35,81) | 54 (36,48) | 0,02 |
| Dislipidemia, n (%) | 175 (21,90) | 47 (26,85) | 80 (45,71) | 48 (27,42) | 0,07 |
| Hábito alcohólico, n (%) | 64 (8,01) | 21 (7,9) | 18 (5,7) | 25 (11,4) | 0,06 |
| Fumador/hábito tabáquico, n (%) | 234 (29,28) | 63 (23,7) | 87 (27,7) | 84 (38,4) | <0,01 |
| Estado de vacunación, n (%) | 0,40 | ||||
| No vacunados | 616 (77,01) | 205 (33,28) | 251 (40,75) | 160 (26) | |
| Vacunación incompleta | 32 (4) | 10 (31,25) | 10 (31,25) | 12 (37,5) | |
| Vacunación completa | 151 (18,90) | 51 (33,77) | 53 (35,01) | 47 (31,12) | |
Los porcentajes de variables del total de la cohorte se muestran sobre el total de la cohorte: porcentaje de columna. Los porcentajes de variables por tercil de costo se muestran sobre el porcentaje de cada variable estudiada: porcentaje de fila. a, b, c: valores con letras diferentes indican diferencias significativas entre los grupos (p<0,01), en la comparación post-hoc con corrección de Bonferroni.
ERC: enfermedad renal crónica; HTA: hipertensión arterial; SOFA: Sequential Organ Failure Assessment; UCI: unidad de cuidados intensivos.
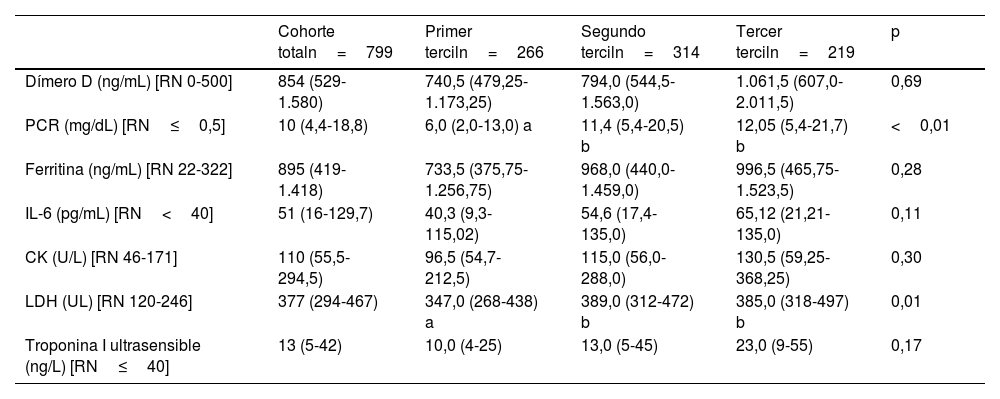
En cuanto a los biomarcadores, se observaron diferencias significativas en la proteína C reactiva (p<0,01) y la lactato deshidrogenasa (p=0,01) (tabla 2).
Biomarcadores inflamatorios y de lesión tisular de la cohorte analizada y según el tercil de coste hospitalario
| Cohorte totaln=799 | Primer terciln=266 | Segundo terciln=314 | Tercer terciln=219 | p | |
|---|---|---|---|---|---|
| Dímero D (ng/mL) [RN 0-500] | 854 (529-1.580) | 740,5 (479,25-1.173,25) | 794,0 (544,5-1.563,0) | 1.061,5 (607,0-2.011,5) | 0,69 |
| PCR (mg/dL) [RN≤0,5] | 10 (4,4-18,8) | 6,0 (2,0-13,0) a | 11,4 (5,4-20,5) b | 12,05 (5,4-21,7) b | <0,01 |
| Ferritina (ng/mL) [RN 22-322] | 895 (419-1.418) | 733,5 (375,75-1.256,75) | 968,0 (440,0-1.459,0) | 996,5 (465,75-1.523,5) | 0,28 |
| IL-6 (pg/mL) [RN<40] | 51 (16-129,7) | 40,3 (9,3-115,02) | 54,6 (17,4-135,0) | 65,12 (21,21-135,0) | 0,11 |
| CK (U/L) [RN 46-171] | 110 (55,5-294,5) | 96,5 (54,7-212,5) | 115,0 (56,0-288,0) | 130,5 (59,25-368,25) | 0,30 |
| LDH (UL) [RN 120-246] | 377 (294-467) | 347,0 (268-438) a | 389,0 (312-472) b | 385,0 (318-497) b | 0,01 |
| Troponina I ultrasensible (ng/L) [RN≤40] | 13 (5-42) | 10,0 (4-25) | 13,0 (5-45) | 23,0 (9-55) | 0,17 |
Los datos se expresan como mediana (p25-p75). a, b, c: valores con letras diferentes indican diferencias significativas entre los grupos (p<0,05), en la comparación post-hoc con corrección de Bonferroni.
CK: creatina cinasa; IL-6: interleucina-6; LDH: lactato deshidrogenasa; PCR: proteína C reactiva; RN: rango de referencia de normalidad.
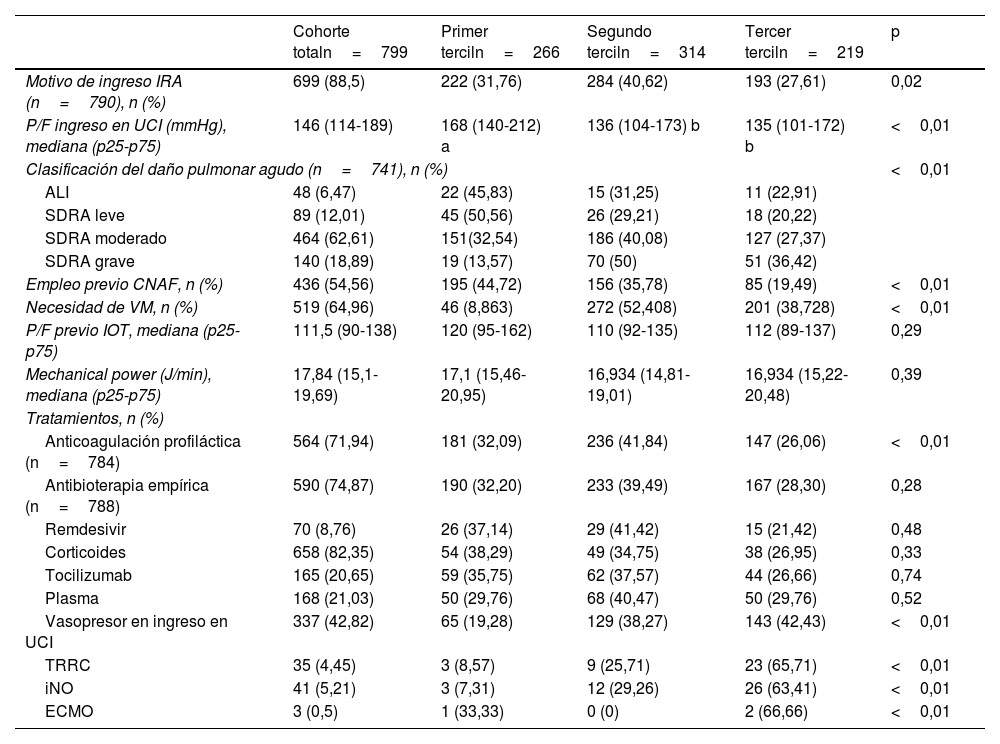
El principal motivo de ingreso en UCI fue la insuficiencia respiratoria aguda (88,5%), con diferencias significativas entre los terciles (p=0,02). El índice presión arterial de oxígeno/fracción inspiratoria de oxígeno al ingreso fue menor en el segundo y tercer tercil en comparación con el primero (p<0,01). La mayoría de los pacientes presentaron síndrome de dificultad respiratoria aguda moderado (62,61%), con un aumento de la gravedad en los terciles superiores (p<0,01). El empleo de cánulas nasales de alto flujo durante el ingreso en UCI-COVID fue más frecuente en el primer tercil (44,72%), disminuyendo progresivamente en los siguientes (p<0,01). La necesidad de ventilación mecánica (VM) (64,96%) mostró diferencias significativas entre terciles (p<0,01), siendo mayor en el segundo y tercero (tabla 3).
Principales variables relacionadas con la insuficiencia respiratoria y los tratamientos empleados durante el ingreso en UCI-COVID de la cohorte analizada y según el tercil de coste hospitalario
| Cohorte totaln=799 | Primer terciln=266 | Segundo terciln=314 | Tercer terciln=219 | p | |
|---|---|---|---|---|---|
| Motivo de ingreso IRA (n=790), n (%) | 699 (88,5) | 222 (31,76) | 284 (40,62) | 193 (27,61) | 0,02 |
| P/F ingreso en UCI (mmHg), mediana (p25-p75) | 146 (114-189) | 168 (140-212) a | 136 (104-173) b | 135 (101-172) b | <0,01 |
| Clasificación del daño pulmonar agudo (n=741), n (%) | <0,01 | ||||
| ALI | 48 (6,47) | 22 (45,83) | 15 (31,25) | 11 (22,91) | |
| SDRA leve | 89 (12,01) | 45 (50,56) | 26 (29,21) | 18 (20,22) | |
| SDRA moderado | 464 (62,61) | 151(32,54) | 186 (40,08) | 127 (27,37) | |
| SDRA grave | 140 (18,89) | 19 (13,57) | 70 (50) | 51 (36,42) | |
| Empleo previo CNAF, n (%) | 436 (54,56) | 195 (44,72) | 156 (35,78) | 85 (19,49) | <0,01 |
| Necesidad de VM, n (%) | 519 (64,96) | 46 (8,863) | 272 (52,408) | 201 (38,728) | <0,01 |
| P/F previo IOT, mediana (p25-p75) | 111,5 (90-138) | 120 (95-162) | 110 (92-135) | 112 (89-137) | 0,29 |
| Mechanical power (J/min), mediana (p25-p75) | 17,84 (15,1-19,69) | 17,1 (15,46-20,95) | 16,934 (14,81-19,01) | 16,934 (15,22-20,48) | 0,39 |
| Tratamientos, n (%) | |||||
| Anticoagulación profiláctica (n=784) | 564 (71,94) | 181 (32,09) | 236 (41,84) | 147 (26,06) | <0,01 |
| Antibioterapia empírica (n=788) | 590 (74,87) | 190 (32,20) | 233 (39,49) | 167 (28,30) | 0,28 |
| Remdesivir | 70 (8,76) | 26 (37,14) | 29 (41,42) | 15 (21,42) | 0,48 |
| Corticoides | 658 (82,35) | 54 (38,29) | 49 (34,75) | 38 (26,95) | 0,33 |
| Tocilizumab | 165 (20,65) | 59 (35,75) | 62 (37,57) | 44 (26,66) | 0,74 |
| Plasma | 168 (21,03) | 50 (29,76) | 68 (40,47) | 50 (29,76) | 0,52 |
| Vasopresor en ingreso en UCI | 337 (42,82) | 65 (19,28) | 129 (38,27) | 143 (42,43) | <0,01 |
| TRRC | 35 (4,45) | 3 (8,57) | 9 (25,71) | 23 (65,71) | <0,01 |
| iNO | 41 (5,21) | 3 (7,31) | 12 (29,26) | 26 (63,41) | <0,01 |
| ECMO | 3 (0,5) | 1 (33,33) | 0 (0) | 2 (66,66) | <0,01 |
Los porcentajes de variables del total de la cohorte se muestran sobre el total de la cohorte: porcentaje de columna. Los porcentajes de variables por tercil de costo se muestran sobre el porcentaje de cada variable estudiada: porcentaje de fila. a, b, c: valores con letras diferentes indican diferencias significativas entre los grupos (p<0,05), en la comparación post-hoc con corrección de Bonferroni.
ALI: lesión pulmonar aguda; CNAF: cánulas nasales de alto flujo; ECMO: oxigenación por membrana extracorpórea; iNO: óxido nítrico inhalado; IOT: intubación orotraqueal; IRA: insuficiencia respiratoria aguda; P/F: ratio presión arterial de oxígeno/fracción inspiratoria de oxígeno; SDRA: síndrome de dificultad respiratoria aguda; TRRC: terapia de remplazo renal continua; UCI: unidad de cuidados intensivos; VM: ventilación mecánica.
La anticoagulación profiláctica se administró en el 71,94% de los pacientes, con diferencias entre terciles (p<0,01), mientras que la antibioterapia empírica no mostró diferencias relevantes. El uso de vasopresores al ingreso fue más frecuente en el tercer tercil (p<0,01). Los tratamientos avanzados, como terapia continua de remplazo renal, óxido nítrico inhalado y membrana de oxigenación extracorpórea, se emplearon con mayor frecuencia en los pacientes encuadrados en el tercer tercil de coste, con diferencias significativas (p<0,01) (tabla 3).
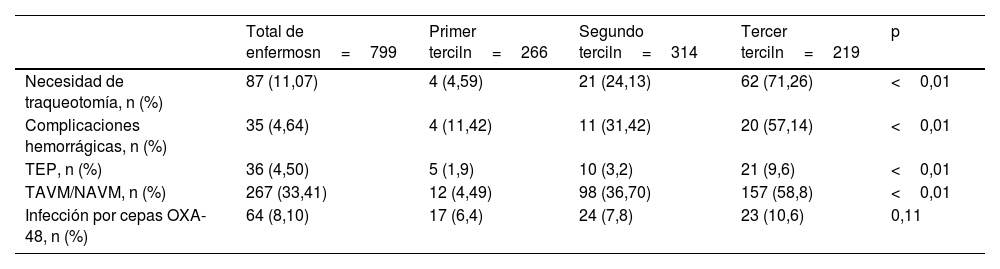
Los principales efectos adversos no deseados durante el ingreso en UCI-COVID de la cohorte analizada, según la categorización por terciles de coste hospitalario, se muestran en la tabla 4.
Principales efectos adversos no deseados durante el ingreso en UCI-COVID de la cohorte analizada y según la categorización por terciles de coste hospitalario
| Total de enfermosn=799 | Primer terciln=266 | Segundo terciln=314 | Tercer terciln=219 | p | |
|---|---|---|---|---|---|
| Necesidad de traqueotomía, n (%) | 87 (11,07) | 4 (4,59) | 21 (24,13) | 62 (71,26) | <0,01 |
| Complicaciones hemorrágicas, n (%) | 35 (4,64) | 4 (11,42) | 11 (31,42) | 20 (57,14) | <0,01 |
| TEP, n (%) | 36 (4,50) | 5 (1,9) | 10 (3,2) | 21 (9,6) | <0,01 |
| TAVM/NAVM, n (%) | 267 (33,41) | 12 (4,49) | 98 (36,70) | 157 (58,8) | <0,01 |
| Infección por cepas OXA-48, n (%) | 64 (8,10) | 17 (6,4) | 24 (7,8) | 23 (10,6) | 0,11 |
Los porcentajes de variables del total de la cohorte se muestran sobre el total de la cohorte: porcentaje de columna. Los porcentajes de variables por tercil de costo se muestran sobre el porcentaje de cada variable estudiada: porcentaje de fila.
OXA-48: oxacilinasa 48; TAVM/NAVM: traqueobronquitis/neumonía asociadas a ventilación mecánica; TEP: tromboembolismo pulmonar.
Por otro lado, se observó un incremento significativo en los días de VM a medida que se avanzaba en los terciles de coste, con una mediana de 2 días (p25-p75: 0-7) en el primer tercil, 7 días (p25-p75: 4-11) en el segundo y 16 días (p25-p75: 10-29,25) en el tercero (p<0,01). La estancia en UCI-COVID también mostró un patrón de aumento progresivo, con medianas de 4 días (p25-p75: 2-6) en el primer tercil, 9 días (p25-p75: 6-13) en el segundo y 20 días (p25-p75: 14-35) en el tercero (p<0,01). De manera similar, la estancia hospitalaria total se incrementó significativamente, con medianas de 11 días (p25-p75: 9-15), 17 días (p25-p75: 13-24) y 28 días (p25-p75: 22-41) en los respectivos terciles (p<0,01).
En cuanto a la mortalidad, los pacientes en el primer tercil presentaron tasas considerablemente menores en comparación con los demás grupos. La mortalidad a los 28 días fue del 9,46% en el primer tercil, frente al 47,30% en el segundo y el 43,24% en el tercero (p<0,01). Esta tendencia se mantuvo en la mortalidad a 60 días (7,00: 40,00 y 53,00%, respectivamente; p<0,01) y a 90 días (6,93; 39,60 y 53,47%, respectivamente; p<0,01).
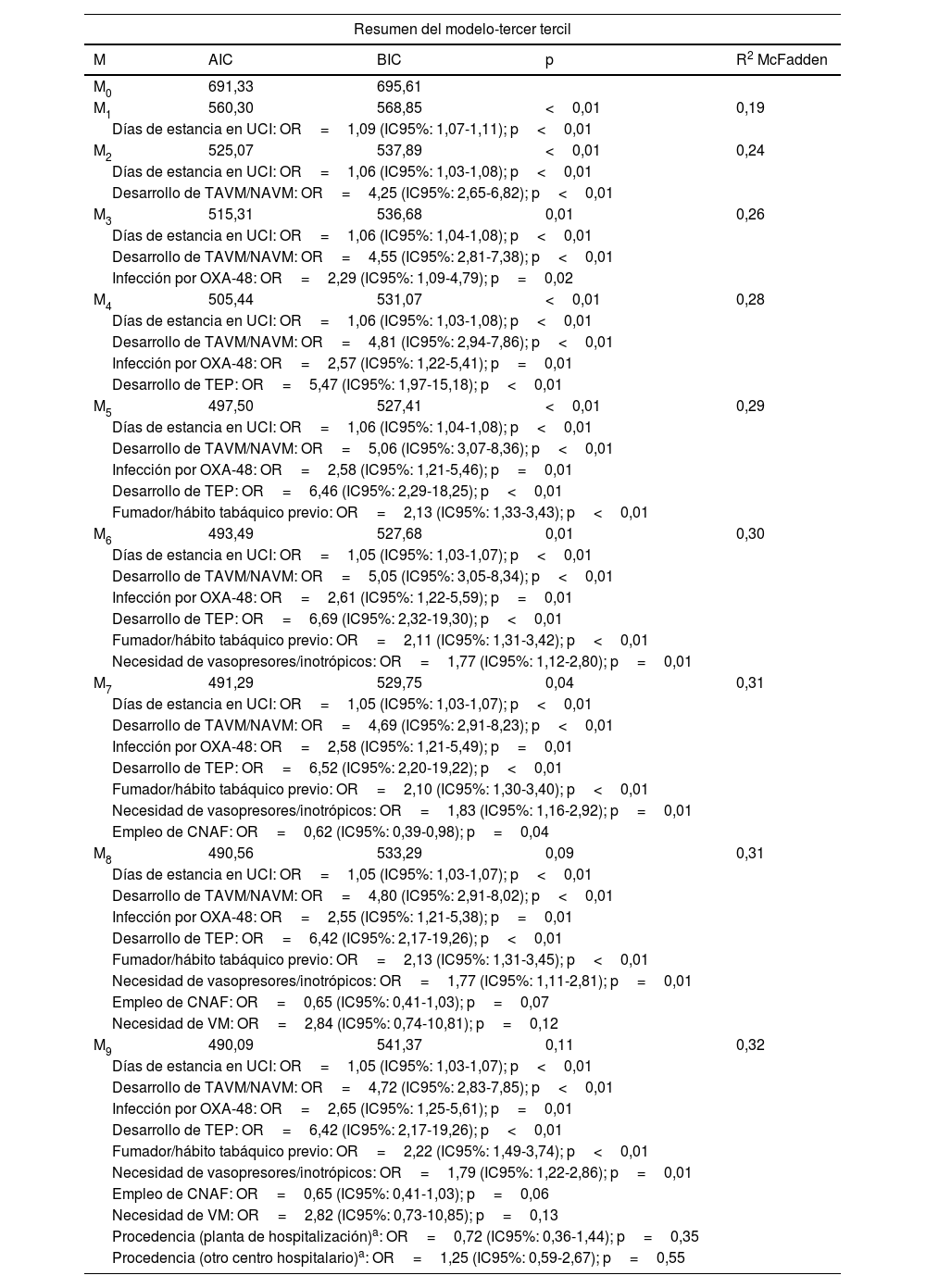
Modelos de regresión logísticaAl añadir los días de estancia en UCI (M1), el AIC bajó a 560,30, el BIC a 568,85 (p<0,01) y el R2 de McFadden alcanzó 0,19, con una OR de 1,09 (IC 95%: 1,07-1,11; p<0,01). En M2, al incluir además el desarrollo de traqueobronquitis/neumonía asociadas a ventilación mecánica (TAVM/NAVM), el AIC descendió a 525,07, el BIC a 537,89 (p<0,01) y el R2 subió a 0,24; las OR fueron 1,06 (IC 95%: 1,03-1,08; p<0,01) para la estancia en UCI y 4,25 (IC 95%: 2,65-6,82; p<0,01) para TAVM/NAVM. Con la adición de infección por OXA-48 en M3, el AIC se situó en 515,31 y el BIC en 536,68 (p=0,01; R2=0,26), obteniendo una OR de 1,06 (IC 95%: 1,04-1,08; p<0,01) para estancia, 4,55 (IC 95%: 2,81-7,38; p<0,01) para TAVM/NAVM y 2,29 (IC 95%: 1,09-4,79; p=0,02) para OXA-48. Al incorporar el desarrollo de tromboembolismo pulmonar (TEP) en M4, el AIC bajó a 505,44 y el BIC a 531,07 (p<0,01; R2=0,28), con OR de 1,06 (IC 95%: 1,03-1,08; p<0,01) para estancia, 4,81 (IC 95%: 2,94-7,86; p<0,01) para TAVM/NAVM, 2,57 (IC 95%: 1,22-5,41; p=0,01) para OXA-48 y 5,47 (IC 95%: 1,97-15,18; p<0,01) para TEP. La inclusión del hábito tabáquico en M5 redujo aún más el AIC a 497,50 y el BIC a 527,41 (p<0,01; R2=0,29), añadiendo un OR de 2,13 (IC 95%: 1,33-3,43; p<0,01). Al sumar la necesidad de vasopresores/inotrópicos en M6, el AIC fue 493,49 y el BIC 527,68 (p=0,01; R2=0,30), con una OR de 1,77 (IC 95%: 1,12-2,80; p=0,01). En M7 incorporamos el empleo de cánulas nasales de alto flujo, obteniendo un AIC de 491,29, un BIC de 529,75 (p=0,04; R2=0,31) y una OR de 0,62 (IC 95%: 0,39-0,98; p=0,04). Finalmente, la adición de la necesidad de VM en M8 (AIC=490,56; BIC=533,29; p=0,09; R2=0,31) y de la procedencia del ingreso (planta u otro centro) en M9 (AIC=490,09; BIC=541,37; p=0,11; R2=0,32) no aportó mejoras significativas ni predictoras adicionales relevantes (tabla 5).
Modelos de regresión logística
| Resumen del modelo-tercer tercil | ||||
|---|---|---|---|---|
| M | AIC | BIC | p | R2 McFadden |
| M0 | 691,33 | 695,61 | ||
| M1 | 560,30 | 568,85 | <0,01 | 0,19 |
| Días de estancia en UCI: OR=1,09 (IC95%: 1,07-1,11); p<0,01 | ||||
| M2 | 525,07 | 537,89 | <0,01 | 0,24 |
| Días de estancia en UCI: OR=1,06 (IC95%: 1,03-1,08); p<0,01 | ||||
| Desarrollo de TAVM/NAVM: OR=4,25 (IC95%: 2,65-6,82); p<0,01 | ||||
| M3 | 515,31 | 536,68 | 0,01 | 0,26 |
| Días de estancia en UCI: OR=1,06 (IC95%: 1,04-1,08); p<0,01 | ||||
| Desarrollo de TAVM/NAVM: OR=4,55 (IC95%: 2,81-7,38); p<0,01 | ||||
| Infección por OXA-48: OR=2,29 (IC95%: 1,09-4,79); p=0,02 | ||||
| M4 | 505,44 | 531,07 | <0,01 | 0,28 |
| Días de estancia en UCI: OR=1,06 (IC95%: 1,03-1,08); p<0,01 | ||||
| Desarrollo de TAVM/NAVM: OR=4,81 (IC95%: 2,94-7,86); p<0,01 | ||||
| Infección por OXA-48: OR=2,57 (IC95%: 1,22-5,41); p=0,01 | ||||
| Desarrollo de TEP: OR=5,47 (IC95%: 1,97-15,18); p<0,01 | ||||
| M5 | 497,50 | 527,41 | <0,01 | 0,29 |
| Días de estancia en UCI: OR=1,06 (IC95%: 1,04-1,08); p<0,01 | ||||
| Desarrollo de TAVM/NAVM: OR=5,06 (IC95%: 3,07-8,36); p<0,01 | ||||
| Infección por OXA-48: OR=2,58 (IC95%: 1,21-5,46); p=0,01 | ||||
| Desarrollo de TEP: OR=6,46 (IC95%: 2,29-18,25); p<0,01 | ||||
| Fumador/hábito tabáquico previo: OR=2,13 (IC95%: 1,33-3,43); p<0,01 | ||||
| M6 | 493,49 | 527,68 | 0,01 | 0,30 |
| Días de estancia en UCI: OR=1,05 (IC95%: 1,03-1,07); p<0,01 | ||||
| Desarrollo de TAVM/NAVM: OR=5,05 (IC95%: 3,05-8,34); p<0,01 | ||||
| Infección por OXA-48: OR=2,61 (IC95%: 1,22-5,59); p=0,01 | ||||
| Desarrollo de TEP: OR=6,69 (IC95%: 2,32-19,30); p<0,01 | ||||
| Fumador/hábito tabáquico previo: OR=2,11 (IC95%: 1,31-3,42); p<0,01 | ||||
| Necesidad de vasopresores/inotrópicos: OR=1,77 (IC95%: 1,12-2,80); p=0,01 | ||||
| M7 | 491,29 | 529,75 | 0,04 | 0,31 |
| Días de estancia en UCI: OR=1,05 (IC95%: 1,03-1,07); p<0,01 | ||||
| Desarrollo de TAVM/NAVM: OR=4,69 (IC95%: 2,91-8,23); p<0,01 | ||||
| Infección por OXA-48: OR=2,58 (IC95%: 1,21-5,49); p=0,01 | ||||
| Desarrollo de TEP: OR=6,52 (IC95%: 2,20-19,22); p<0,01 | ||||
| Fumador/hábito tabáquico previo: OR=2,10 (IC95%: 1,30-3,40); p<0,01 | ||||
| Necesidad de vasopresores/inotrópicos: OR=1,83 (IC95%: 1,16-2,92); p=0,01 | ||||
| Empleo de CNAF: OR=0,62 (IC95%: 0,39-0,98); p=0,04 | ||||
| M8 | 490,56 | 533,29 | 0,09 | 0,31 |
| Días de estancia en UCI: OR=1,05 (IC95%: 1,03-1,07); p<0,01 | ||||
| Desarrollo de TAVM/NAVM: OR=4,80 (IC95%: 2,91-8,02); p<0,01 | ||||
| Infección por OXA-48: OR=2,55 (IC95%: 1,21-5,38); p=0,01 | ||||
| Desarrollo de TEP: OR=6,42 (IC95%: 2,17-19,26); p<0,01 | ||||
| Fumador/hábito tabáquico previo: OR=2,13 (IC95%: 1,31-3,45); p<0,01 | ||||
| Necesidad de vasopresores/inotrópicos: OR=1,77 (IC95%: 1,11-2,81); p=0,01 | ||||
| Empleo de CNAF: OR=0,65 (IC95%: 0,41-1,03); p=0,07 | ||||
| Necesidad de VM: OR=2,84 (IC95%: 0,74-10,81); p=0,12 | ||||
| M9 | 490,09 | 541,37 | 0,11 | 0,32 |
| Días de estancia en UCI: OR=1,05 (IC95%: 1,03-1,07); p<0,01 | ||||
| Desarrollo de TAVM/NAVM: OR=4,72 (IC95%: 2,83-7,85); p<0,01 | ||||
| Infección por OXA-48: OR=2,65 (IC95%: 1,25-5,61); p=0,01 | ||||
| Desarrollo de TEP: OR=6,42 (IC95%: 2,17-19,26); p<0,01 | ||||
| Fumador/hábito tabáquico previo: OR=2,22 (IC95%: 1,49-3,74); p<0,01 | ||||
| Necesidad de vasopresores/inotrópicos: OR=1,79 (IC95%: 1,22-2,86); p=0,01 | ||||
| Empleo de CNAF: OR=0,65 (IC95%: 0,41-1,03); p=0,06 | ||||
| Necesidad de VM: OR=2,82 (IC95%: 0,73-10,85); p=0,13 | ||||
| Procedencia (planta de hospitalización)a: OR=0,72 (IC95%: 0,36-1,44); p=0,35 | ||||
| Procedencia (otro centro hospitalario)a: OR=1,25 (IC95%: 0,59-2,67); p=0,55 | ||||
AIC: criterio de información de Akaike; BIC: criterio de información de Bayes; CNAF: cánulas nasales de alto flujo; IC95%: intervalo de confianza del 95%; OR: odds ratio; OXA-48: oxacilinasa 48; TAVM/NAVM: traqueobronquitis/neumonía asociadas a ventilación mecánica; TEP: tromboembolismo pulmonar; UCI: unidad de cuidados intensivos; VM: ventilación mecánica.
El área bajo la curva obtenida fue de 0,866, con un valor de p<0,01 (fig. 2).
Discusión
A pesar de que los cuidados críticos suponen una importante carga de costes sanitarios, se publican relativamente pocos estudios de costo en cuidados críticos (un promedio de 4,6 estudios por año), y la tendencia actual es el uso de cohortes hipotéticas y escenarios de modelado sin datos clínicos comprobados9.
El presente trabajo identifica un conjunto de variables relacionadas con el ingreso en una UCI-COVID que, de forma independiente, se asocian con los enfermos que tuvieron un mayor coste hospitalario. Entre ellas se incluyen la duración de la estancia en UCI, el desarrollo de TAVM/NAVM, la infección por OXA-48, la presencia de TEP, el antecedente de hábito tabáquico y la necesidad de vasopresores o inotrópicos.
De nuestro análisis surgen algunas evidencias que, aunque previsibles, no dejan de ser relevantes y pueden generar un interesante debate. Un ejemplo claro es la relación entre la duración de la estancia en la UCI-COVID y el costo hospitalario: que los días de hospitalización en UCI sean un factor independiente para predecir mayores costos es un hecho ampliamente documentado, dado que los recursos necesarios –incluyendo la dotación de personal, el uso de medicamentos y los procedimientos diagnósticos– representan aproximadamente el 20% del gasto hospitalario total10. Un estudio francés realizado antes de la pandemia ya había identificado el tiempo de estancia en una cama de UCI como un determinante independiente del costo hospitalario (r=0,716; p<0,0001)11. En este contexto, es importante señalar que estudios europeos en países como Francia y Alemania han evidenciado que la mayor parte de los costos en UCI (hasta un 62%) están directamente relacionados con la dotación de personal y el nivel hospitalario12.
Por otro lado, para entender la estimación del incremento de costes debidos a un aumento en la estancia a causa de eventos adversos –TAVM/NAVM, TEP, infección por OXA-48– durante la permanencia en la UCI, es crucial entender la exposición como un factor que varía en el tiempo para evitar un sesgo temporal que ocurre cuando asumimos implícitamente que las condiciones están presentes desde el ingreso, lo que lleva a una sobredistensión del efecto incremental. En este sentido, Bluhmki et al. fueron conscientes de este problema y estimaron correctamente el exceso de estancia hospitalaria asociado con la NAVM utilizando modelos de estados múltiples que tienen en cuenta la dinámica temporal del estado de ventilación y la aparición de NAVM. Al mismo tiempo, Bluhmki et al. consideraron que ignorar la dependencia temporal de la NAVM llevaría a estimar un exceso de estancia de 15 días, lo que representa una sobrestimación sustancial en comparación con la estimación más precisa de 3,52 días. Esto también podría ocurrir en estudios como el nuestro, en el que, aunque se disponga de datos de costos, la omisión de la dependencia temporal de la exposición podría haber llevado a una sobrestimación significativa del efecto real13,14.
Los resultados en la bibliografía subrayan la VM como un impulsor importante de los costos de la UCI (aumento cercano al 30%), aunque muestran una variabilidad sustancial de los costos para diferentes enfermedades subyacentes y eventos adversos en los entornos de la UCI15,16. En el caso del síndrome de dificultad respiratoria aguda, pequeñas reducciones en la duración de la estadía en la UCI pueden beneficiar a los pacientes, pero no conducen a reducciones significativas en los costos hospitalarios generales. El alta temprana a centros de cuidados postagudos puede reducir los costos hospitalarios, pero es poco probable que reduzca significativamente los costos de un episodio completo de enfermedad17.
El TEP fue una complicación estrechamente relacionada con la enfermedad por COVID-19, destacándose como un factor diferencial en la fisiopatología del síndrome de dificultad respiratoria aguda asociado al virus. Esta particularidad no solo influyó en la gravedad y evolución clínica de los pacientes, sino que también tuvo implicaciones en el manejo terapéutico. En la literatura previa a la pandemia, se describe el TEP como una afección donde los costos de enfermería constituyen el componente más importante, muy por encima de los costes de farmacia y radiología, similares en ambos casos. Sin embargo, otros 2 aspectos a considerar son, por un lado, que los costos del tratamiento durante el primer año después del alta hospitalaria son altos, y por otro, que una carga creciente de enfermedades comórbidas se asocia fuertemente con un aumento del costo real de la atención de pacientes hospitalizados por TEP18–20.
Desde una perspectiva de economía de la salud, las infecciones por bacterias productoras de OXA-48 se inscriben dentro del desafío más amplio de las infecciones por patógenos multirresistentes. Diversos estudios han demostrado que el coste asistencial de los pacientes con infecciones por bacterias resistentes es significativamente superior al de aquellos con infecciones por patógenos susceptibles. Este incremento se atribuye a una mayor duración de la enfermedad, la necesidad de pruebas diagnósticas adicionales, estancias hospitalarias prolongadas, el uso de antimicrobianos de alto coste y una mayor tasa de mortalidad21. La magnitud del problema es considerable: las infecciones por microorganismos resistentes podrían generar una reducción del 1,1% del producto interno bruto global y, en un escenario de bajo impacto, ocasionar pérdidas económicas superiores a un billón de dólares anuales después de 2030. En este contexto, una estimación precisa de la carga asociada a estas infecciones es fundamental para diseñar estrategias eficaces de prevención y control, permitiendo una asignación racional de los recursos sanitarios. La literatura ha demostrado con evidencia sólida que ciertas intervenciones, como la implementación de programas de gestión del uso de antimicrobianos, son eficaces para mejorar el cumplimiento de una prescripción racional y reducir tanto el uso como la duración de la terapia antibiótica, lo que conlleva una disminución en la estancia hospitalaria y en los costes21,22.
En relación con el hábito tabáquico, un trabajo realizado desde el inicio de la pandemia hasta el 15 de julio de 2020 en un hospital español evidenció que los pacientes fumadores presentaron una mayor incidencia de complicaciones durante su estancia hospitalaria, especialmente complicaciones relacionadas con el sistema respiratorio y cardíaco. También se asociaron a un peor pronóstico en cuanto a necesidad de ingreso en UCI y mortalidad, lo que supuso un aumento del coste de gestión de los pacientes fumadores con COVID-19 en un 14,72%23. En el mismo sentido, otros trabajos comprobaron que ser fumador o exfumador también se asoció con costos diarios más elevados24.
Este estudio presenta varias limitaciones. En primer lugar, su diseño retrospectivo y unicéntrico puede limitar la generalización de los hallazgos a otros hospitales con distinta estructura de costes y manejo clínico. Además, la categorización del coste hospitalario mediante APR-GRD, si bien es una herramienta ampliamente utilizada, podría no captar todas las particularidades del consumo de recursos en UCI-COVID. Asimismo, no se consideraron factores sociales o del entorno que podrían influir en la duración de la estancia y los costes. Finalmente, no se puede descartar la presencia de factores de confusión residuales no contemplados en el modelo.
AutoríaAlejandro González-Castro: ideación, elaboración y redacción del manuscrito.
Carmen Huertas: ideación del texto, depuración de base de datos, recogida de datos.
Trinidad Dierssen Soto: análisis estadístico.
Elena Cuenca Fito: recogida de datos.
Yhivian Peñasco: elaboración, corrección.
Reinhard Wallmann: recogida de datos.
Raquel Ferrero Franco: depuración de base de datos.
Juan Carlos Rodríguez Borregán: elaboración, corrección.
Fuente de financiaciónEl trabajo presentado no ha tenido ninguna fuente de financiación.
Declaración sobre el uso de la IA generativa y de las tecnologías asistidas por la IA en el proceso de redacciónPara la redacción y síntesis de este manuscrito, hemos utilizado inteligencia artificial como apoyo en la estructuración del texto y la mejora de su claridad y coherencia. En particular, hemos empleado ChatGPT. La interpretación de los datos, el análisis crítico y las conclusiones del estudio han sido desarrollados íntegramente por los autores.
Conflicto de interesesLos autores declaran no tener conflictos de intereses con la realización de este trabajo.

