





On November 3, 2019, a 34-year-old woman in cardiac arrest (CA) due to accidental hypothermia was transferred to Hospital Universitario Vall d’Hebron, Barcelona, Catalonia, Spain. The patient was rescued in the Pyrenees with an initial esophageal temperature of 19.4 °C, initial rhythm of asystole, cyanosis in acral parts, and bilateral unresponsive mydriasis. The first venous blood gas revealed: pH levels of 6.8, potassium levels of 4.6, and lactate levels of 10.3. A HOPE score of 88% was calculated, which led to the indication of extracorporeal life support (ECLS) with venoarterial extracorporeal membrane oxygenation (VA-ECMO) via ipsilateral right femoro-femoral surgical cannulation. After gradual rewarming at a rate of 3 °C/h, spontaneous circulation was restored after defibrillation once the central temperature exceeded 30 °C. The patient progressed favorably, which eventually led to removing ECMO support 45 h later. The patient was eventually discharged 11 days later with a Cerebral Performance Category of 1.1,2
To date, another case of CA due to accidental hypothermia resuscitated for 3 h had been published in Medicina Intensiva in Spain, but it was an in-hospital CA, and no previous experiences of extracorporeal cardiopulmonary resuscitation (ECPR) had ever been reported in these patients.3
The initially reported case represents the first successful resuscitation in Spain of an out-of-hospital CA patient due to accidental hypothermia and the longest resuscitation published nationally. Nearly 5 years after the accident, the patient is in excellent general condition. To evaluate functionality in activities of daily living, a Barthel test was performed which showed a score of 100/100. Additionally, a multidimensional quality of life test perceived by the person was performed too (the World Health Organization Quality of Life scale abbreviated – WHOQOL-BREF). A psychologist reviewed the test, which revealed a total score of 125/130 (10/10, general area; 34/35, physical; 26/30, psychological; 15/15, social; 40/40, environmental). These data demonstrate that recovery after such a long resuscitation has been complete and reintegration into a normal life in all areas has been successful.
In Catalonia, Spain more than 19,000 rescues have been reported in the natural environment since 2010, with almost 50% being mountain rescues.4 In the past 2 decades, there have been other cases of CA due to accidental hypothermia. With the authorization of the ethics committee of hospital Arnau de Vilanova (CEIC-1308) and the analysis of the reports from the Mountain Intervention Unit of Mossos d’Esquadra and the Mountain Rescue Group of Bombers d'Andorra, all fatal accidents due to accidental hypothermia in the Pyrenees of Catalonia and Andorra from 2000 through 2024 have been compiled (Table 1). A total of 29 cases have been documented so far. Of these, 65.5% involved men, with a median age of 40 years (IQR, 35–48). A total of 48.2% of the cases occurred outside the winter season. The most practiced activity was ski mountaineering, followed by hiking, with most cases occurring in the Ripollés region (51.7%) and Val d’Aran (24.1%). No CPR measures were initiated in 69% of the victims, and only 4 victims (13.8%) were transferred to an ECMO center. Grouping data by number of reported accidents, a total of 17 accidents occurred (6 in winter, 5 in autumn, 4 in summer, and 2 in spring). These data indicate that 64.7% of the accidents occurred in non-winter seasons.
Cases of accidental hypothermia* in the Pyrenees of Catalonia and Andorra from 2000 through 2024.
| Victim | Age | Sex | Location | Region | Activity | Season | Accident date | Mechanism | CPR or ECLS attempt | Transfer to an ECMO-capable center | Survivor |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 51 | M | Balandrau | Ripollès | Ski Mountaineering | Winter | 30/12/2000 | Accidental | No | No | No |
| 2 | 37 | M | Balandrau | Ripollès | Ski Mountaineering | Winter | 30/12/2000 | Accidental | No | No | No |
| 3 | 35 | M | Balandrau | Ripollès | Ski Mountaineering | Winter | 30/12/2000 | Accidental | No | No | No |
| 4 | 37 | M | Balandrau | Ripollès | Ski Mountaineering | Winter | 30/12/2000 | Accidental | No | No | No |
| 5 | 48 | F | Balandrau | Ripollès | Ski Mountaineering | Winter | 30/12/2000 | Accidental | No | No | No |
| 6 | 28 | F | Balandrau | Ripollès | Ski Mountaineering | Winter | 30/12/2000 | Accidental | No | No | No |
| 7 | 37 | F | Balandrau | Ripollès | Ski Mountaineering | Winter | 30/12/2000 | Accidental | No | No | No |
| 8 | 46 | M | Balandrau | Ripollès | Ski Mountaineering | Winter | 30/12/2000 | Accidental | No | No | No |
| 9 | 38 | M | Balandrau | Ripollès | Ski Mountaineering | Winter | 30/12/2000 | Accidental | No | No | No |
| 10 | 44 | M | Costabona | Ripollès | Ski Mountaineering | Winter | 20/1/2001 | Avalanche | No | No | No |
| 11 | 40 | M | Costabona | Ripollès | Ski Mountaineering | Winter | 20/1/2001 | Avalanche | No | No | No |
| 12 | 44 | M | Fontnegra | Ripollès | Ski Mountaineering | Winter | 24/1/2002 | Avalanche | No | No | No |
| 13 | 37 | M | Urús | Cerdanya | Unknown | Spring | 11/4/2004 | Accidental | No | No | No |
| 14 | 50 | F | Restanca | Val d'Aran | Ski Mountaineering | Winter | 15/02/2005 | Accidental | No | No | No |
| 15 | 60 | M | Aiguestortes | Val d'Aran | Ski Mountaineering | Winter | 18/2/2005 | Accidental | No | No | No |
| 16 | 45 | F | Puigmal | Ripollès | Hiking | Autumn | 7/11/2009 | Accidental | No | No | No |
| 17 | 43 | F | Puigmal | Ripollès | Hiking | Autumn | 7/11/2009 | Accidental | Yes, CPR | No | No |
| 18 | 48 | F | Cavalls de vent | Berguedà | Mountain Race | Autumn | 29/9/2012 | Accidental | Yes, CPR | No | No |
| 19 | 35 | M | Andorra | Andorra | Hiking | Winter | 27/12/2012 | Accidental | No | No | No |
| 20 | 43 | M | Cavalls de vent | Berguedà | Mountain Race | Spring | 28/4/2015 | Accidental | Yes, CPR | Yes (renal replacement theraphy machine) | No |
| 21 | 67 | M | Pica d'estats | Pallars Sobirà | Hiking | Summer | 21/08/2015 | Accidental | No | No | No |
| 22 | 28 | M | Circ de Colomers | Val d'Aran | Hiking | Summer | 12/9/2017 | Accidental | Yes, CPR | No | No |
| 23 | 20 | M | Andorra | Andorra | Hiking | Autumn | 29/10/2018 | Accidental | Yes, CPR | No | No |
| 24 | 34 | F | Fontalba | Ripollès | Hiking | Autumn | 4/11/2019 | Accidental | Yes, ECLS | Yes (VA-ECMO) | Yes |
| 25 | 38 | M | Andorra | Andorra | Hiking | Summer | 30/7/2020 | Accidental | Yes, CPR | No | No |
| 26 | 27 | M | Aiguestortes | Val d'Aran | Hiking | Autumn | 25/9/2020 | Accidental | No | No | No |
| 27 | 27 | F | Aiguestortes | Val d'Aran | Hiking | Autumn | 25/9/2020 | Accidental | No | No | No |
| 28 | 65 | M | Aiguestortes | Val d'Aran | Hiking | Summer | 14/9/2022 | Accidental | Yes, ECLS | Yes (VA-ECMO) | No |
| 29 | 69 | F | Aiguestortes | Val d'Aran | Hiking | Summer | 14/9/2022 | Accidental | Yes, ECLS | Yes (VA-ECMO) | No |
CPR, cardiopulmonary resuscitation; ECLS, extracorporeal life support; ECMO, extracorporeal membrane oxygenation; F, female; M, male; VA, venoarterial.
These results should warn us on the de-seasonalization of accidents due to accidental hypothermia and the need for careful evaluation of each case by personnel trained in hypothermia. Currently, hypothermia remains a poorly recognized entity with many biases in its assessment and management.5 Without the presence of environmental cold or a triggering environment (high mountains, drowning, or snowy terrain), hypothermia can be difficult to suspect. However, hypothermia exists in our environment, both in rural and urban settings, and failing to consider it can lead to underdiagnosis. In turn, the most severe cases could be dismissed for transfer to an ECLS center due to lack of knowledge or protocols.
Some specific cases—like the one initially presented in this article—demonstrate the possibility of surviving an out-of-hospital CA due to accidental hypothermia despite the presence of typical markers of poor prognosis in normothermia (asystole, acidosis, lactate, end-tidal carbon dioxide, CA duration, unresponsive mydriasis). Out of all the cases that were not resuscitated, it is impossible to know if their prognosis would have changed or if CPR should have been initiated. However, same as it happens with very specific conditions for which there care and referral circuits remain available such as stroke, acute myocardial infarction, burns, or acute spinal injury, victims of accidental hypothermia should be taken care of through standardized circuits in centers with resources and experience proportional to the risk of CA.
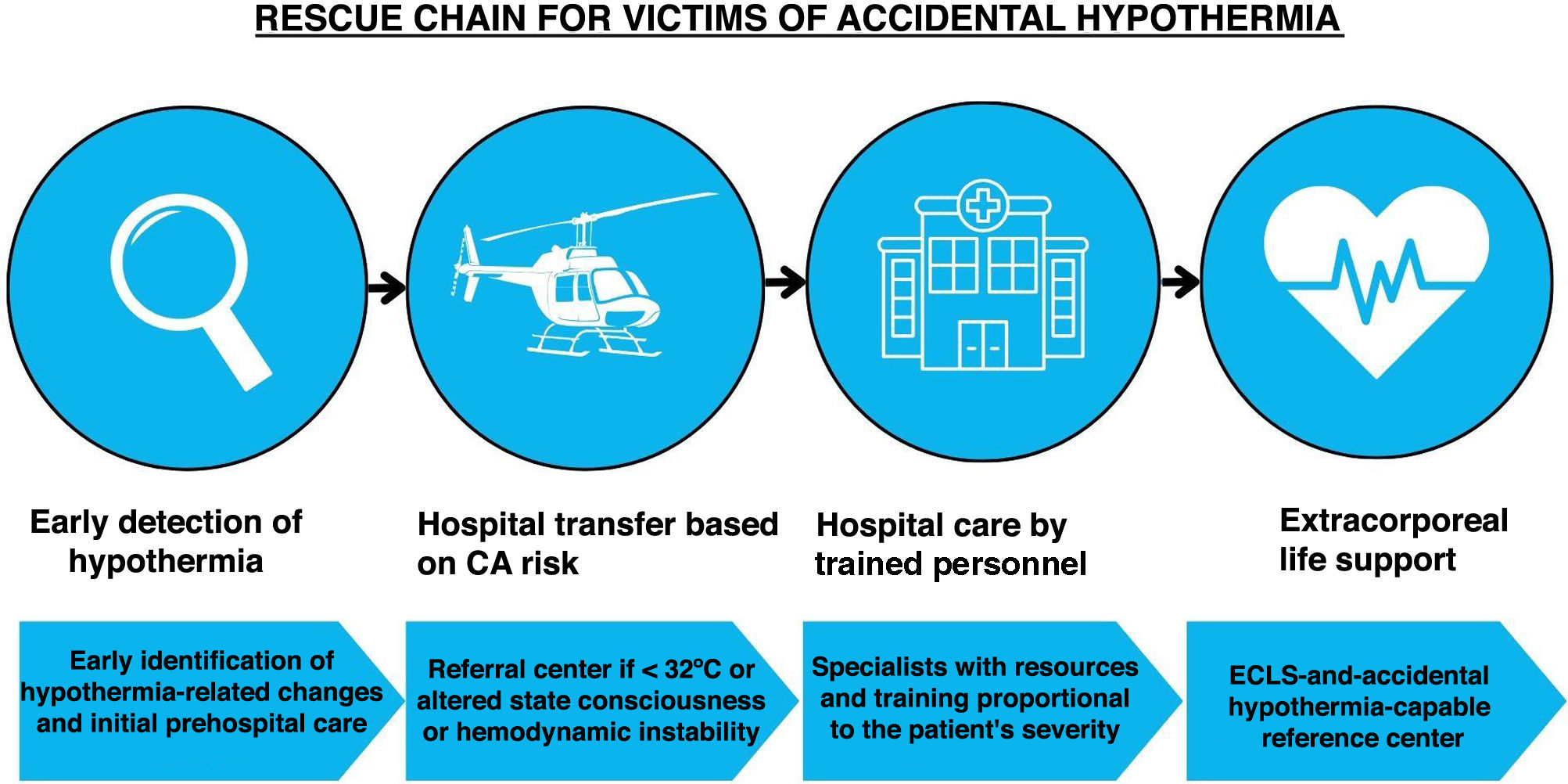
Therefore, a feasible solution would be to implement a specific rescue chain ranging from prehospital services trained in detection, triage, and initial management to, if necessary, transfer to a reference hospital center capable of managing cases of accidental hypothermia with an altered state of consciousness, hemodynamic instability, or temperature ≤30 °C in adults and ≤32 °C in elderly patients with comorbidities (Fig. 1).6–8 A reference center should be equipped with trained and experienced health care personnel in the management of these cases and, also, with specific treatment protocols and circuits, including ECLS, to shorten transfer times by not having to decide which center to refer to while offering the highest possible quality of care.9,10
The approach to this problem can go beyond hospital strategies, providing the first responder with the necessary basics to act and alert. Prevention strategies (providing the victim or responders with the skills needed to resolve the problem when it arises through strategies like informational pamphlets at key points, training courses, information on social networks), prevention campaigns (informational panels, accessible weather information, or preventive advertising campaigns), and intervention strategies (to avoid recurrence of cases, such as improving signals, expanding and securing telephone coverage areas, or improving the traceability of hikers between shelters) can improve the safety of any victim.
Accidental hypothermia is a poorly recognized entity requiring specific management. A total of 86.2% of the victims of all accidents compiled were not transferred to an ECLS-capable center. One out of 3 patients who were put on ECMO survived with excellent functional capacity. The creation of specific circuits associated with reference hypothermia centers should facilitate triage decisions and ensure the proportionality of resources applicable to the risk of CA in any hypothermia victim.
All authors reviewed and approved the final version of the manuscript.
FundingThe authors declare that they have no funding sources to declare.
Authors’ contributionsRobert Blasco was involved in the conceptualization, research, and drafting of the original manuscript, review, and editing.
Eduard Argudo was involved in the conceptualization, drafting, review, and editing of the manuscript.
Iñigo Soteras was involved in the conceptualization, drafting, review, and editing of the manuscript.
Conflicts of interestNone declared. The authors also declare that they have the CEIC approval and the patient’s explicit informed consent for the publication of the case.
The authors wish to thank the members of the Mountain Intervention Unit of the Mossos d'Esquadra, Pompiers de la Val d'Aran, and Mountain Rescue Group of Bombers d'Andorra for their diligent acquisition of records.
Please cite this article as: Blasco Mariño R, Argudo E and Soteras Martinez I. Antes y después de la primera reanimación cardiopulmonar extracorpórea por hipotermia accidental en España, Med Intensiva. 2024. https://doi.org/10.1016/j.medin.2024.05.021

