





The use of restraints in the pediatric setting is still under discussion due to the negative connotations of violating the children’s rights and the stressing effects derived from using these measures in the pediatric patient.1,2 During the comprehensive care of the child, especially pediatric children, it may necessary to use several procedures, techniques, and interventions that can cause pain, physical distress or even great psychological stress. Added to the fact that the child is totally unaware of the procedure or technique being used, this physical and psychological distress limits his cooperation efforts.
The use of physical and mechanical restraint systems at the Pediatric Intensive Care Units (PICU) happens in 2 very different settings: to perform one-time painful procedures and to maintain life support devices (Table 1).
Settings and definitions of the use of restraint systems in the pediatric setting.
| Settings for the use of these systems | Type of restraint system | Definition |
|---|---|---|
| To perform one-time urgent procedures such as venipunctures or starting IVs safely and in a controlled way | Physical restraint by the parents or healthcare providers by immobilizing the limb to be punctured or using full body restraint | In the pediatric setting, the definition of physical restraint to perform a procedure is variable and the distinctive aspect here is exerting the necessary strength to perform the procedure, and whether the minor has given his consent. In this sense, we may have denominations such as therapeutic, clinical or supportive holding or restraint.1,2 |
| - Supportive holding: «positioning without active resistance and with the child and the parents’ consent to perform the medical or clinical procedure safely and in a controlled way». | ||
| - Restraint: «forced immobilization to make sure that the procedure or the technique gets done while always taking into consideration the child’s interest». | ||
| It is discussed whether this different terminology can lead to a somehow “humanization” of the intervention that can mask its consequences since supportive holding has more positive connotations than restraint. | ||
| To make sure that life support devices like endotracheal tubes, vascular catheters, cannulas or drainage tubes are properly maintained | Mechanical restraint | «Actions or procedures aimed at restraining a person’s free movement to a position of his choice or normal access to his body through the use of methods adjacent to a person’s body that he/she can’t control or get rid of easily»3 |
| It includes, among others, the use of gloves, wristbands or chest or abdominal restraint systems |
However, the effectiveness of the use of mechanical restraint systems3 to stop the child from self-removing these devices is still uncertain. Its use could be justified after reviewing each case individually only, when all the other restraints measures have been tried and keeping this measure as a last resource.4,5 In Spain the registries on the use of restraint systems in children admitted to PICUs are scarce though it is a common practice.6 A retrospective trial reported a prevalence of use of mechanical restraint systems of 96% in children between 5 days and 14 years old being hand restraint6 92%. Outside our own country, an international multicenter trial that surveyed 872 healthcare providers to determine how were children contained while performing painful clinical procedures showed that 48% of them used restraint systems often and 33% very often. At the same time, the trial reported that this practice varies significantly depending on the country, profession, clinical experience on this area, training, and availability of alternatives at the working place.7 Similarly, a study among 28 British PICUs showed that 68% of these units used mechanical restraint systems including hand contention measures or splints to avoid joint movement or small mechanical devices like wristbands.8 Unfortunately, we do not know whether these different prevalence among the PICUs has to do with different perspectives from the healthcare providers or with structural (nurse/patient ratio) or clinical issues (work dynamics, management of analgosedation) in these units. Dolz et al.6 say that there is not much information on mechanical restraint systems in the pediatric patient from the clinical point of view (pediatric restraint systems appear nowhere in the documentation, prescription or formal consent form) or in the references. This procedure is defined as “an informal standard of care usually performed by nurses by consensus not because it has been scientifically proven that its benefits exceed its physical, psychological, ethical, and legal repercussions.”
Pediatric nurses have mixed emotions about mechanical restraints. For some, these measures cause more stress in the child than the pain associated with the procedure. At the same time, they put confidence on pediatric care at risk. Others see mechanical restraint systems as an acceptable and unavoidable method, a “reasonable damage” compared to the benefit derived from the therapies.2 It is at this point that we should think about whether the decision to use mechanical restraint systems should fall on one professional only or be an interdisciplinary decision to be made with shared responsibility within the working team.9
The perception of children and their families on the use of these restraint systems is described as “one of the toughest experiences ever lived,” causing great physical and emotional distress.2 In its report, the Joint Commission documented up to 128 adverse events associated with mechanical restraint systems including physical damage and even the death of patients. In this sense, Demir et al.10 describe the appearance of adverse events in PICUs in children carriers of mechanical restraint systems such as edema, limb cyanosis, refusal to eat and agitation. Similarly, the use of mechanical restraint has been associated with a higher risk of delirium and signs of post-traumatic stress disorder at ICU discharge. That is why it is advisable to avoid these measures,11 but this has not been studied in the pediatric setting yet.
Also, we do not really know what impact the physical immobilization derived from these mechanical restraint systems has on the child’s cognitive, psychological, physical, and motor development or at any stage of his development. That is why it is mandatory to not use these systems routinely and analyze each case individually. Also, see what level of understanding the child has, how he expresses himself, whether he is collaborative or not, and what other alternatives are available.12
Immobilizing their kids is emotionally stressful for the parents. In general, they express the need to “be there” and collaborate providing information and wellbeing, distraction and emotional support. However, although they try to leave their emotions behind to not influence their kids’ responses, sometimes they show feelings of moral stress, uncertainty, guilt, and even irritation towards the healthcare providers for breaking the maternal/paternal protective link with the child.7
Therefore, considering the scarce evidence available, adverse events, and negative effects that restraint systems have on children and their families, it is advisable to use other preventive approaches like negotiating—adapting the speech to the age of the child and the parents—and being with the family; methods of distraction like music, early mobilization, early withdrawal of unnecessary devices or the administration of analgosedation in scheduled procedures should make the use of mechanical restraint systems the very last resource.1–5
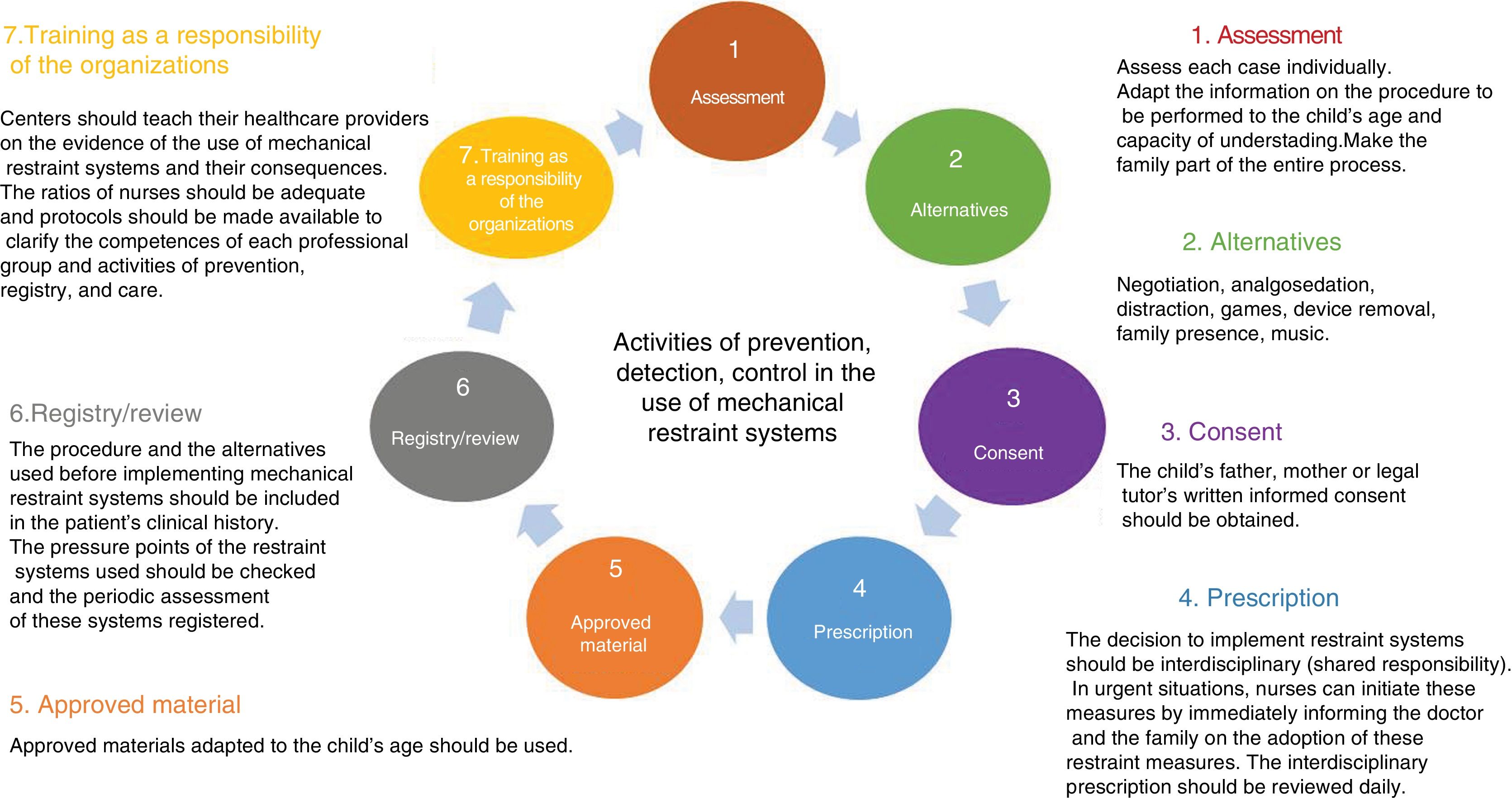
If, even after including the preventive activities already mentioned, the child still needs to be restrained, then the recommendations shown on Fig. 1 should apply.
We need more trials comparing risks, benefits and negative effects derived from using these restraint systems, and strategies to regulate this practice in the pediatric setting in order to minimize the use of physical and mechanical restraint measures and protect the interests and rights of children admitted to these pediatric units.
Conflicts of interestNone reported.
Please cite this article as: Bosch-Alcaraz A, Via-Clavero G. ¿Está justificado el uso de contenciones físicas y mecánicas en el paciente pediátrico ingresado en una unidad de cuidados intensivos? Med Intensiva. 2020;44:192–195.

