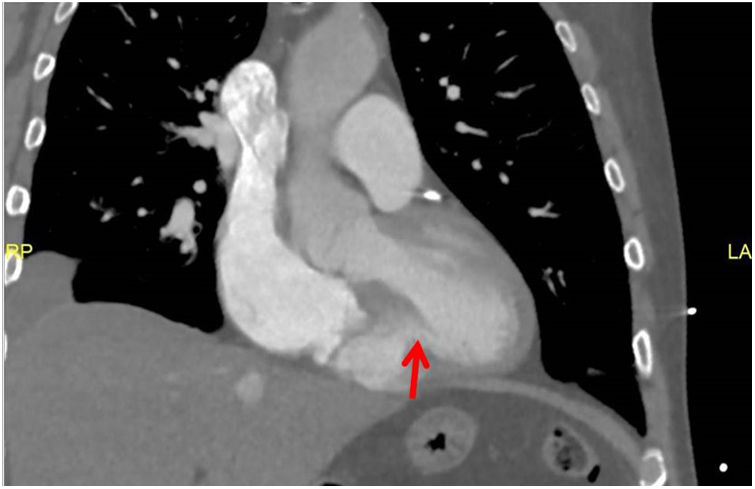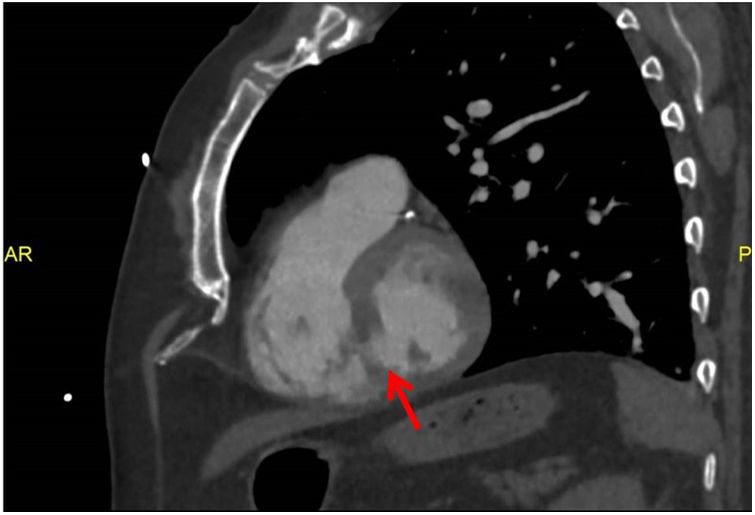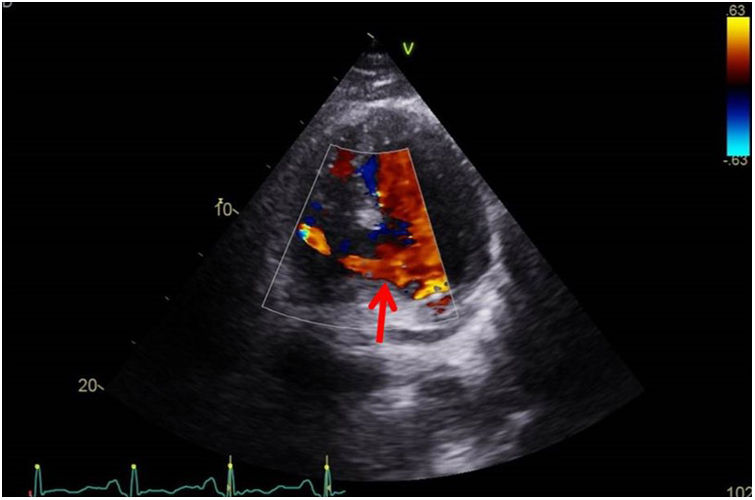
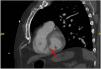
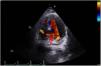
This is the case of a 65-year-old male admitted due to progressive dyspnea of a 20-day history. He is admitted with clinical signs of cardiogenic shock and an unknown panfocal systolic murmur. Complementary tests are performed. The ECG reveals the presence of 1 mm ST-segment depression from V3 to V6 and Q-wave in the inferior wall. Troponin-T levels are 1100 pg/L. The bedside echocardiogram (TTE) performed reveals the presence of right ventricular dilatation with severe tricuspid regurgitation. A coronary computed tomography angiography (CCTA) is, then, performed. The CCTA rules out pulmonary embolism. However, it confirms the presence of ventricular septal rupture (Figs. 1 and 2). A repeat TTE confirms the finding, most likely due to an evolved acute myocardial infarction (Fig. 3). Given the situation of cardiogenic shock, the patient is, then, transferred for veno-arterial extracorporeal membrane oxygenation (ECMO). This case shows the utility of the CT scan to assess complications associated with ischemic heart disease, particularly when the TTE offers diagnostic uncertainties or suboptimal imaging.
Impact factor
The Impact Factor measures the average number of citations received in a particular year by papers published in the journal during the two preceding years.
© Clarivate Analytics, Journal Citation Reports 2025
Impact factor 2024
3.1
View more metrics