








Falls from heights are a major preventable cause of morbidity and mortality in children. The aims of this study are to describe the evolution and long-term prognosis of such patients, to identify the pediatric population at greatest risk of falling from heights in our setting, and to define the variables at admission capable of predicting mortality.
DesignA retrospective patient cohort review was carried out.
SettingPediatric patients.
PopulationPediatric patients admitted to the Pediatric Intensive Care Unit following a fall from a height of over 2m, in the last 10 years.
ResultsNinety-two percent of the patients fell from buildings. Out of a total of 54 patients suffering falls, 51% were preschoolers. Fifty percent of the adolescents cases corresponded to attempted suicide. Fifty-two percent of the children were immigrants. Head injuries were the most common type of traumatism. The mortality rate was 12%. Eighty-two percent of the patients with a follow-up period of 2 years were leading an independent life. The independent predictors of mortality were the height of the fall, the Glasgow coma score and pediatric trauma index score upon admission, the presence of anemia, acidosis and hypotension upon admission, the need for vasoactive drugs, and the presence of severe head injury with the development of intracranial hypertension.
ConclusionsFalls from heights occur mainly in unsupervised preschool children and teenagers attempting suicide. These patients have a high number of injuries, a high mortality rate, and important care needs. Most survivors are able to lead an independent life over the long term. Preventive measures should be implemented in risk populations.
Las caídas desde altura son una importante causa de morbimortalidad prevenible en la edad pediátrica. Los objetivos de este estudio son describir la evolución y el pronóstico a largo plazo de los pacientes precipitados, identificar la población pediátrica con mayor riesgo de sufrir caídas desde altura en nuestro medio y definir las variables al ingreso asociadas a mortalidad.
DiseñoEstudio de una cohortes retrospectivo.
ÁmbitoPediatría.
ParticipantesPacientes politraumatizados ingresados en el servicio de Unidad de Cuidados Intensivos Pediátricos tras haberse precipitado desde una altura superior a dos metros a lo largo de 10 años.
ResultadosEl 92% de las caídas se produjeron desde edificios. De 54 pacientes precipitados, el 51% fueron preescolares. En adolescentes, el intento de suicidio ha sido la causa en la mitad de los casos. Un 52% pertenece a familias inmigrantes. El traumatismo craneoencefálico fue la lesión más frecuente. La mortalidad fue del 12%. De los pacientes en los que se realizó seguimiento a los dos años, el 82% llevaban una vida independiente sin secuelas. Los factores independientes asociados a mortalidad fueron: la altura de la caída, la puntuación en la Escala de Coma de Glasgow y en el Índice de Trauma Pediátrico, la anemia, la acidosis y la hipotensión al ingreso, la necesidad de drogas vasoactivas, y la presencia de TCE grave con desarrollo de hipertensión intracraneal.
ConclusionesLas caídas desde grandes alturas se producen sobre todo en preescolares sin supervisión y en adolescentes por tentativa de suicidio. Estos pacientes presentan un gran número de lesiones, una alta mortalidad y altas necesidades asistenciales. La mayoría de los supervivientes llevan una vida independiente a largo plazo. Sería necesario implantar medidas preventivas, sobre todo en la población de riesgo.
Accidental falls from heights are among the leading causes of death and permanent brain and bone damage in children.1 “Falls from a height” are generally taken to represent falls from a height of over 2m.
In the United States, the annual incidence of falls from buildings is 2.81 per 100,000 inhabitants,2–5 reaching rates of 37 per 100,000 inhabitants in developing countries.6–10 There are no incidence or prevalence data for Spain.
Falls from heights are the most frequent cause of emergency department consultations due to trauma (995 cases per 100,000 subjects under 18 years of age annually),11,12 and are considered to be the fourth most common cause of trauma-related death after traffic accidents, burns and drowning.13–15 The percentage mortality rate referred to falls from a height among pediatric patients is 5.9% in the developed world.16 Thirty-three percent of the serious head injuries recorded in infants under 2 years of age in Spain are due to falls from a height.17 Ninety-five percent of these children fall from buildings, particularly in the warm months and in the late afternoon hours.
The height from which the victims fall, the presence of head injuries, and findings indicative of poor prognosis upon admission are the main mortality predictors in children suffering falls from a height.18 Some population-based studies define age, gender and a low socioeconomic level as independent risk factors for accidents of this kind.19
The Children Can’t Fly program in the United States proved able to lower the proportion of children falling from buildings by 96%.20,21
Although there are no incidence data in our setting, falls from a height are an important cause of preventable morbidity–mortality in the pediatric population. The aim of the present study is to describe the lesions profile, the medical care needs, the complications and the long-term prognosis of fall victims admitted to a Pediatric Intensive Care Unit (PICU) during the last decade. It also aims to identify the pediatric population at greatest risk of suffering falls from a height in our setting, and to define the variables upon admission capable of predicting mortality in these patients.
Patients and methodsA review was made of the cohort of polytraumatized children admitted to the PICU of Niño Jesus University Children's Hospital, a pediatric polytraumatism reference unit in the Community of Madrid (Spain), covering the period between August 2001 and August 2010. The study included those children in which the mechanism of injury was a fall from a height of over 2m. The data were obtained by reviewing the clinical histories and through telephone interviews of the patients or their parents.
Personal data were collected, along with information referred to disease and social antecedents of interest, if any. Regarding the fall, we documented the time and place of the accident, the people accompanying the children at the time, the presence or absence of buffering of the fall, and who provided first care. Certain vital signs and laboratory test values recorded at the time of first care were analyzed: the venous bicarbonate and pH values (acidosis being regarded as a venous pH of under 7.20), hemoglobin (Hb) concentration (the cutoff point for defining anemia being Hb <9g/dl), blood pressure (BP) (hypotension being defined by a systolic BP value below percentile 5 for the age of the patient), and transcutaneous oxygen saturation (SatO2). As severity markers we included the need for intubation, the Pediatric Trauma Score (PTS) upon admission,22 the score on the Glasgow Coma Scale (GCS) modified for pediatrics, and the need for vasoactive drugs and blood products. As outcome variables we analyzed the type of patient lesions, the need of surgery, the days of stay in Intensive Care, and mortality. In those cases where it proved possible, we documented the score of the Glasgow Outcome Scale (GOS) after 2 years.23
A study was made of the distribution and frequencies of the different variables, with binary logistic regression analysis, using the chi-squared test with a 95% confidence interval (95% CI), relating mortality to the different variables of each patient. The SPSS version 15.0 statistical package was used throughout.
ResultsEpidemiological characteristicsOf the 443 polytraumatized patients admitted to the PICU in the last decade, 189 (43%) suffered injuries as a consequence of falls. In 54 patients (12%) the height of fall was over 2m.
The mean patient age was 6 years (range 0.4–14 years). Most of the subjects (51%) were pre-school infants, followed by children over 12 years of age (22%). There were no significant gender differences. Fifty-two percent of the children cam from immigrant families, particularly from Latin America (30%), followed by Asians (8%) and Arab countries (5%). In 39% of the families, both parents were unemployed. Most of the children (49%) lived with both parents, and 36% belonged to families with more than four children. Social problems were detected in 13 families.
Two of the patients suffered severe mental retardation, and eight had psychiatric problems.
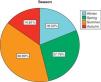
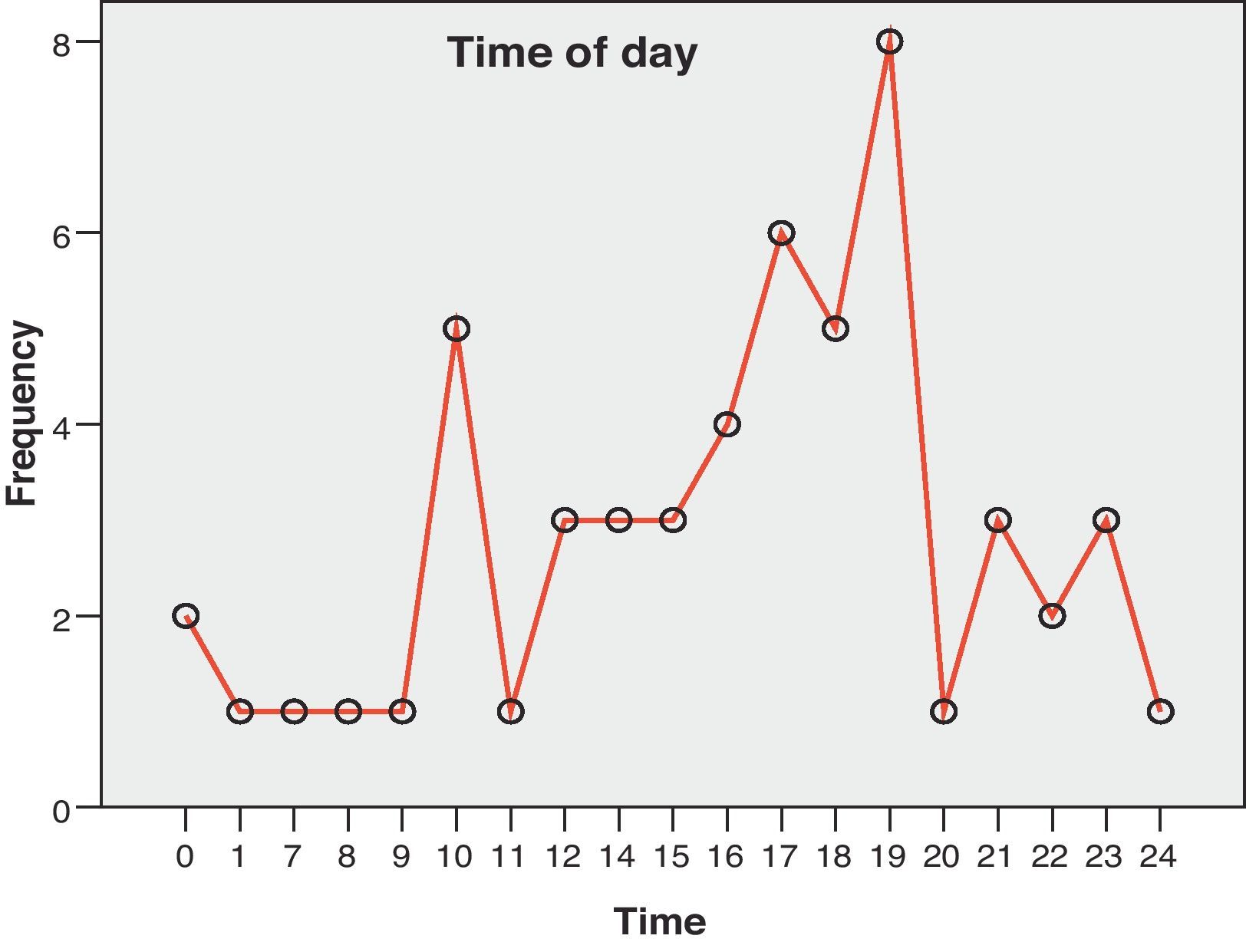
Sixty-six percent of the falls occurred in the warm months of the year (Fig. 1), and between 4 in the afternoon and 9 o’clock at night (Fig. 2). In turn, 92% of the falls were from buildings. None of the families reported having safety mechanisms or systems in their home windows or balconies. Nine falls were buffered by something: clotheslines, trees, roofs, etc. In 70% of the cases the falls were from the home of the victim. Of note is the fact that eight children were accompanied by other children, and 11 were completely alone at home, at the time of the accident. Eight children had climbed onto furniture close to the window. Playing was a frequent cause in all age groups (Fig. 3). Among the adolescents, attempted suicide was the first cause of falls, accounting for 50% of the cases (Fig. 3).
Lesions and outcome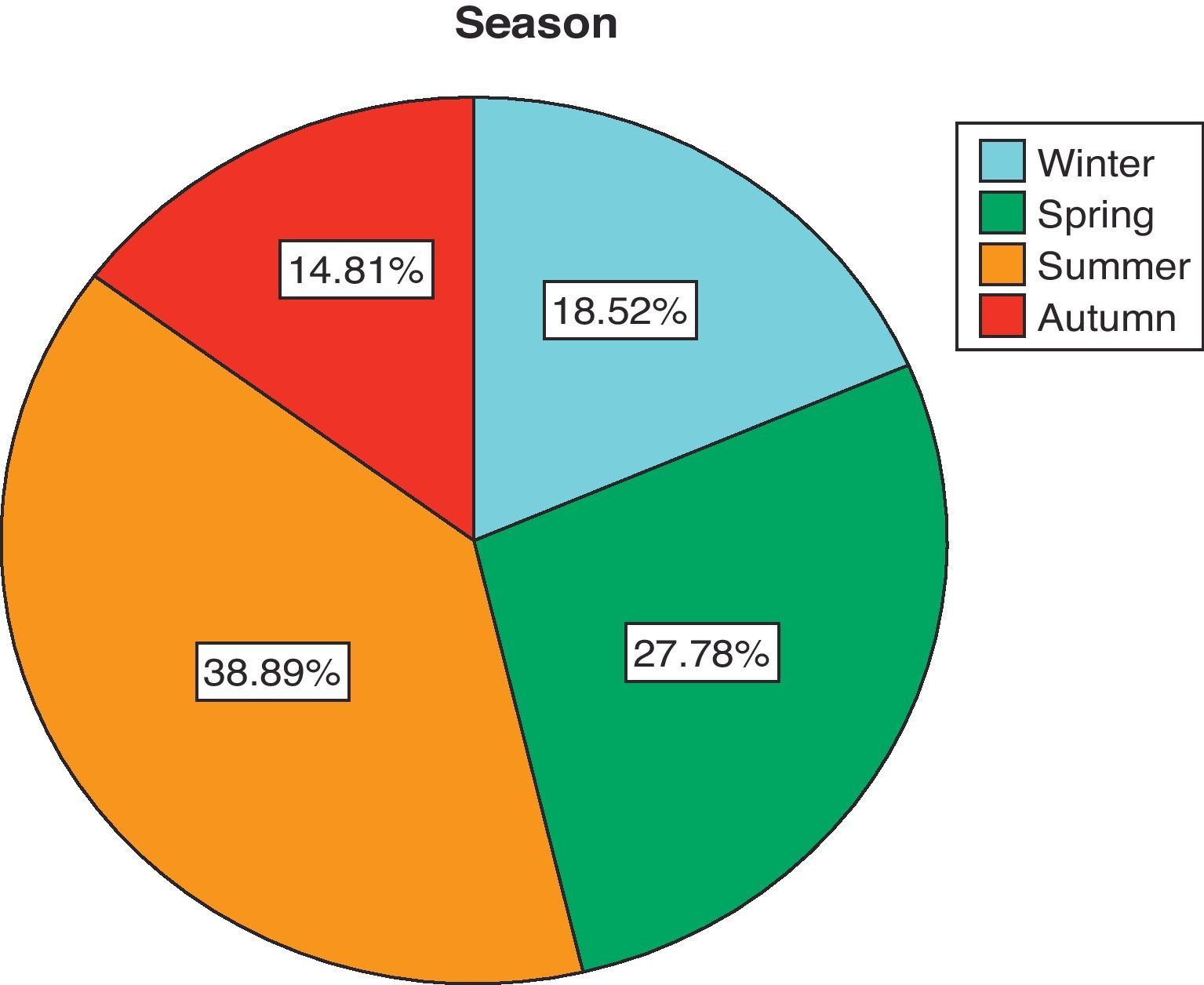
Thirty-four children (63%) were initially attended by the out-hospital medical services. Eighteen patients (33%) were intubated before being taken to hospital, and another six had indications for intubation. Six patients (11%) presented acidosis upon admission, and 17 (31%) had hypotension. The mean GCS score following initial stabilization was 11.7 (3–15). The mean PTS score in the first 24h was 6.91 (−2 to 12). The PTS and GCS scores upon admission were significantly correlated to patient mortality and to prognosis of the outcome at 2 years (Table 1).
Prediction of mortality and Glasgow Outcome Scale at 2 years, with the Pediatric Trauma Score upon admission and Glasgow Coma Scale.
| Mortality | GOS at 2 years | |
| PTS | p: 0.06; 95% CI: 0.577–0.912 | p: 0.02; 95% CI: 0.067–0.273 |
| GCS | p: 0.05; 95% CI: 0.584–0.912 | p: 0.001; 95% CI: 0.107–0.270 |
GCS: Glasgow Coma Scale; GOS: Glasgow Outcome Scale at 2 years; PTS: Pediatric Trauma Score.
Thirty-eight patients (70%) suffered some type of head injury; of these, 15 were serious head injuries (Table 2). There were no differences in the occurrence of head injuries in the different age groups. The computed tomography (CT) study detected intracranial injuries (ICIs) in 24 patients. Fifteen patients (27%) had clinical manifestations consistent with intracranial hypertension (ICH). One patient suffered spinal cord injury. Traumatic lesions were the second in order of frequency (54%). Forty percent of the patients suffered some type of chest injury—particularly lung contusion. Liver damage in turn was the most frequent abdominal injury.
Types of lesions in head injuries.
| Type of lesion | No. patients/% appearancea | No. patients requiring surgery |
| Head injury | 38 (70) | 10 |
| Mild head injury | 12 (22) | |
| Moderate head injury | 11 (20) | |
| Severe head injury | 15 (27) | |
| Cranial fracture | 25 (46) | |
| Brain contusion | 12 (22) | |
| Epidural hematoma | 10 (19) | |
| Subdural hematoma | 8 (15) | |
| Thoracic injury | 22 (40) | 1 |
| Pneumothorax | 3 (5) | |
| Lung contusion | 18 (33) | |
| Rib fracture | 1 (2) | |
| Abdominal injury | 14 (25) | 2 |
| Liver damage | 9 (17) | |
| Pancreatic damage | 2 (4) | |
| Kidney damage | 2 (4) | |
| Traumatologic injury | 27 (51) | 6 |
| Limb fracture | 19 (35) | |
| Pelvic fracture | 4 (7) | |
| Vertebral fracture | 1 (2) | |
| Nasal bone fracture | 1 (2) | |
Total number and percentage appearance with respect to total patients.
Sixty percent of the patients required the transfusion of blood products. In turn, 46% of the patients received volume expansion and 20 were administered vasoactive drugs. Twenty-three patients (42%) required mechanical ventilation (MV), with a mean duration of 5 days (range 3–15 days).
The mean duration of stay among the survivors was 8 days (0–80 days). Of the 40 patients evaluated after 2 years, 33 (82%) were seen to lead an independent life without sequelae (26 patients, GOS=5) or with moderate sequelae (seven patients, GOS=4). Another seven patients (17%) suffered serious sequelae and were totally dependent on others for activities of daily living (seven patients GOS=2 or 3).
Study of mortalitySeven patients died (12%). All fatalities were a consequence of falls from over 9m. The mean PTS score was 2.86 with a range between −2 and 9. The mean GCS score among the deceased patients was 3.8, with a median of 3 (3–5). Three of the patients were transferred under conditions of hypoxemia. The pH value upon admission was under 7.20 in four patients, with a mean of 7.18.
The ultimate causes of death were brain death in two children, hypovolemic shock in another two children, and cardiorespiratory arrest in three patients.
Of all the study variables, only nine showed a statistically significant association to mortality (Table 3).
Variables associated to mortality.
| Statistically significant variables | ||
| Variables | Significance | 95% CI |
| Height of fall | 0.026 | (1.02–1.5) |
| PTS upon admission | 0.006 | (0.572–0.912) |
| GCS upon admission | 0.005 | (0.584–0.912) |
| Appearance of ICH | 0.02 | (1.38–48.1) |
| Acidosis upon admission | 0.01 | (0.01–0.019) |
| Hypotension upon admission | 0.027 | (0.23–0.80) |
| Anemia upon admission | 0.02 | (0.38–0.92) |
| Need for vasoactive drugs | 0.04 | (1.01–36) |
| Presence of head injury | 0.023 | (1.41–115.98) |
Acidosis upon admission: venous pH<7.20; Anemia upon admission: hemoglobin <9g/dl; GCS: Glasgow Coma Scale; Hypotension upon admission: systolic blood pressure<percentile 5 for age; ICH: intracranial hypertension; 95% CI: 95% confidence interval; PTS: Pediatric Trauma Score.
Our study confirms that the immigrant population at social risk and without employment living in buildings with over six floors constitutes the maximum risk group in relation to accidental falls from a height. These results coincide with those reported by other authors.24 In contrast to other series, however, we recorded no greater incidence of falls in large families.4,5,24 There were two age peaks in our series of fall victims that coincide with the data in most of the studies found in the literature.15 The first peak is observed in pre-school children between 2 and 5 years of age. At this age children become independent in terms of mobility but are still unaware of the risks or hazards. Distraction on the part of the care takers, the closeness of furniture to windows, or the assumption that the children are sleeping are all causes of accidental falls in this age group. In the group of adolescents, attempted suicide is seen to predominate in patients with psychiatric problems and depression or chronic illnesses.
The Children Can’t Fly initiative, introduced in the cities of New York and Boston in the 1970s, with the adoption of legislative measures and the application of a program designed to increase awareness of safety measures applied to windows and balconies, was able to produce a very important decrease in the percentage of children falling from buildings. In Spain there have been no such legislative measures or preventive campaigns.20,21 Preventive measures, required in application to the global population, should be intensified in the immigrant population, without employment, and living in tall buildings in the urban setting.
Falls are more common in the late afternoon hours, at a time when the children are at home and many are supposedly sleeping. Another peak in incidence is observed in the morning when the windows are opened for home cleaning purposes. In turn, the spring and summer seasons concentrate two-thirds of these accidents. Preventive strategies therefore should be intensified in these periods.
The present study is unable to offer incidence data, since our hospital does not have a reference population. Falls from any height are the leading cause of polytraumatisms admitted to our Unit (43%), followed by run-over patients (23%), traffic accidents (13%) and bicycle or motorcycle accidents (7.86%). Falls from a height of over 2m considered isolatedly (12.1%) in turn represent the fourth most common cause of admission. These results coincide with the information found in the literature.11–14
Head injuries were the most common type of injury in our series. The younger the child, the larger the head size in comparison with the torso—displacing the body center of gravity in the cephalad direction.19,25 In our study there were no differences in the percentages of head injuries in the different age groups. The high percentage of ICI in our series may be biased by patient severity upon admission, since these were patients admitted to the PICU. The high incidence of limb fractures in the 3–10 years age group is explained by the fact that these children are unable to verticalize on falling, and so fall on their upper and lower extremities.26 Intraabdominal trauma is frequent in children who fall from a height, because the liver and spleen are proportionately larger in relation to body size, and the ribs are more flexible.
The medical care requirements of fall victims are very important. In our series most of the patients required prolonged admission to the PICU, with ventilation and hemodynamic support, the administration of blood products, and surgery.
The mortality rate in our series was 12%, which is higher than in other published series,27 since our study only included patients admitted directly to the PICU from the out-hospital services or second-level hospital centers. Seventeen percent of the survivors suffered serious sequelae with dependency upon others for activities of daily living—this in turn implying an important burden for both the family and the healthcare system.
The factors associated with increased mortality are reported in Table 3. In contrast to other series, age and the need for mechanical ventilation were not identified as mortality indicators.
ConclusionsFalls from heights affect particularly unattended pre-school children and adolescents—the latter in the context of attempted suicide. These patients suffer numerous lesions, especially head injuries, and high mortality, and have important healthcare needs. Most survivors are able to lead an independent life over the long term. The immigrant population without employment and living in buildings with over six floors should be targeted for legislative measures and awareness-enhancing campaigns referred to the adoption of safety measures in windows and balconies.
Conflicts of interestThe authors declare no conflicts of interest.
Please cite this article as: Pérez-Suárez E, et al. Caídas desde grandes alturas en Pediatría. Epidemiología y evolución de 54 pacientes. Med Intensiva. 2012;36:89–94.

