




To describe the incidence of hypophosphatemia in patients admitted to the ICU who have required mechanical ventilation. To analyze the presence of risk factors and its relationship with nutritional practice.
DesignProspective observational study.
SettingPolyvalent ICUs of 2 University Hospitals.
Patients or participantsPatients on invasive mechanical ventilation ≥72 h with normal level of phosphorus at admission.
InterventionsNone.
Main variables of interestElectrolyte levels (phosphorus, magnesium, potassium) were determined on admission to the ICU and at 96 h. Risk categories on admission, caloric intake, insulin doses and acid-base status during the first 4 days of admission were recorded. Incidence was calculated as the number of patients who developed hypophosphataemia after admission. Univariate analysis was performed for between-group comparison and multivariate analysis of potential risk factors.
Results89 patients were included. The incidence of hypophosphataemia was 32.6%. In these patients phosphorus decreased from 3.57 ± 1.02 mmol/l to 1.87 ± 0.65 mmol/l (52.3%). The mean kcal/kg/24 h provided in the first 4 days was 17.4 ± 4.1, with no difference between the group that developed hypophosphataemia and the group that did not. Significant risk factors were insulin doses administered and pH and PaCO2 values.
ConclusionsThe incidence of hypophosphataemia at 96 h from admission in mechanically ventilated patients is high and unrelated to the risk category and hypocaloric nutritional practice used. Insulin dosis and acid-base status are the main determinants of its occurrence.
Describir la incidencia de hipofosfatemia en pacientes ingresados en UCI que han precisado ventilación mecánica. Analizar la presencia de factores de riesgo y la relación con la práctica nutricional realizada.
DiseñoEstudio observacional prospective.
ÁmbitoUcis polivalentes de 2 Hospitales Universitarios.
Pacientes o participantespacientes en ventilación mecánica invasiva ≥72 horas con niveles de fósforo normales al ingreso.
Intervencionesninguna.
Variables de interés principalesSe determinaron los niveles de iones (fósforo, magnesio, potasio) al ingreso en UCI y a las 96 horas. Se registraron las categorias de riesgo al ingreso, el aporte calórico, las dosis de insulina y el estado ácido-base durante los primeros 4 días de ingreso. La incidencia se calculó como el número de pacientes que desarrollaron hipofosfatemia tras el ingreso. Se realizó un análisis univariante para la comparación entre grupos y un multivariante de los potenciales factores de riesgo.
ResultadosSe incluyeron 89 pacientes. La incidencia de hipofosfatemia fue del 32.6%. En estos pacientes el fósforo disminuyó de 3,57 ± 1,02 mmol/l a 1,87 ± 0,65 mmol/l (un 52,3%). La media de kCalorías/kg/24 h aportada en los primeros 4 dias fue de 17.4 ± 4.1, no existiendo diferencias entre el grupo que desarrolló hipofosfatemia y el que no. Los factores de riesgo significativos fueron las dosis de insulina administradas y los valores de pH y PaCO2.
ConclusionesLa incidencia de hipofosfatemia a las 96 horas de ingreso en pacientes con ventilación mecánica es elevada y no guarda relación con la categoría de riesgo y la práctica nutricional hipocalórica utilizada. Las dosis de insulina y el estado ácido-base son sus principales determinantes.
The so-called refeeding syndrome (RS) is a condition described in prisoners of war who, after a prolonged period of starvation, are initiated on feeding.1 The RS is a constellation of primarily cardiovascular, respiratory, neurological, and metabolic symptoms associated with changes to the levels of various electrolytes (phosphate, magnesium, and potassium) and related to the reintroduction of caloric intake, usually nutritionally.2,3 RS is well-documented in certain patient populations, such as those with eating disorders (anorexia), cancer patients with digestive problems, etc., but its existence in critically ill patients is still a matter of discussion.4,5
In critically ill patients on invasive mechanical ventilation, clinical recognition of RS is challenging due to the presence of other multiple causes of the typical signs and symptoms of this entity. Specifically, the 3 most characteristic symptoms (tachycardia, tachypnea, and edema) are entirely nonspecific in this context.6 This requires consideration of its definition based on laboratory abnormalities, primarily the decrease in plasma phosphate levels. Multiple studies have used different cut-off values and ranges of decline, resulting in widely variable incidence rates.7–9 To mitigate this heterogeneity and enable comparisons, a standardized definition was recently established in a consensus conference.10
Various risk factors and risk categories have been proposed for screening and detecting patients with RS. In recent years, new recommendations have been made alongside the classic NICE guidelines,11 including a consensus conference10 and the ASPEN guidelines.12
The aim of this study is to describe the incidence of hypophosphatemia (as an indicator of the RS in critically ill patients on invasive mechanical ventilation and its relationship with the risk categories defined in the consensus conference, caloric intake, and other variables associated with its development.
Patients and methodsThis was a prospective, observational study that included all patients admitted to the polyvalent ICUs of 2 teaching hospitals from the province of Granada, Spain over a 6-month period from July through December 2021 who required a 72-or-more-hour course of respiratory support with invasive mechanical ventilation. Patients with hypophosphatemia in the initial laboratory determination (first 24 h), those with chronic kidney disease, those who developed acute renal failure within the first 72 h, and patients admitted with a diagnosis of diabetic ketoacidosis were excluded.
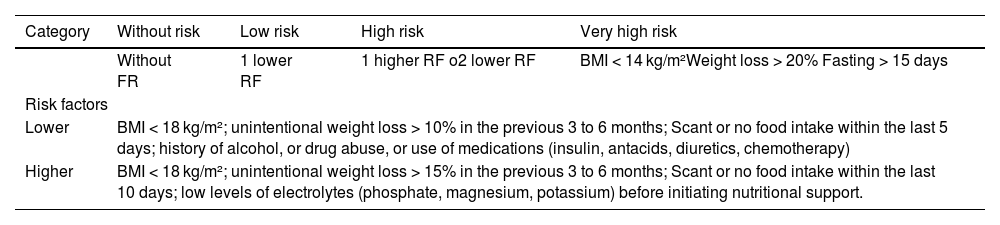
Risk factors for developing RS were recorded and categorized into the risk categories of the consensus conference (none, low, high, and very high) (Table 1). Ion levels (phosphate, magnesium, potassium) were determined at the ICU admission, 96 h later, and on days 7–10. The administration of calories within the first 4 days of admission was recorded, including that provided by glucose solutions and propofol. Both units have a unified protocol for administering and monitoring nutrition in critically ill patients, prioritizing enteral nutrition with initiation within the first 24 h of admission followed by progressive administration within the first 7 days until caloric and protein goals have been reached. These goals were calculated based on the patient's weight, on the phase of critical illness, with 25 kcal/kg/day and 1.3 g/kg/day during the acute phase, and in full compliance with the international recommendations.13 In the case of patients categorized as at risk for the RS, the protocol recommended reducing caloric intake down to 50% of the usual calculated targets.
Categories and risk factors (RF).
| Category | Without risk | Low risk | High risk | Very high risk |
|---|---|---|---|---|
| Without FR | 1 lower RF | 1 higher RF o2 lower RF | BMI < 14 kg/m²Weight loss > 20% Fasting > 15 days | |
| Risk factors | ||||
| Lower | BMI < 18 kg/m²; unintentional weight loss > 10% in the previous 3 to 6 months; Scant or no food intake within the last 5 days; history of alcohol, or drug abuse, or use of medications (insulin, antacids, diuretics, chemotherapy) | |||
| Higher | BMI < 18 kg/m²; unintentional weight loss > 15% in the previous 3 to 6 months; Scant or no food intake within the last 10 days; low levels of electrolytes (phosphate, magnesium, potassium) before initiating nutritional support. | |||
BMI, body mass index; RF, risk factor.
Initially, according to the protocol, the administered diets were standard polymeric enteral formulations. In some patients, after the 4-day study period, these were replaced by special formulations, or adapted to their circumstances. All these diets ensured the daily recommended amounts of electrolytes and oligoelements when the calculated caloric-protein requirements were met.
In addition, 2 other factors known to contribute to the development of hypophosphatemia in critically ill patients were recorded: the mean doses of insulin administered to patients who required it and the mean pH and CO2 levels from all arterial blood samples taken within the first 96 h to assess the impact of respiratory alkalosis.
Hypophosphatemia was defined as phosphate values <0.8 mmol/L, or a decrease of ≥30% between the 2 determinations (at admission and at 72 h). Correction of hypophosphatemia was left to the attending physician’s discretion.
The incidence rate was calculated as the percentage of patients who developed hypophosphatemia after the ICU admission out of the total number of patients. Results are expressed descriptively as means, medians, and proportions. Univariate analysis was performed using the independent samples t-test, while the multivariate analysis was performed using binary logistic regression with backward variable selection. The pH variable was not included in the latter analysis as it was considered related to PaCO2, being the latter indicative of the origin of alkalosis.
The study was approved by the research ethics committee of the province of Granada, Spain and informed consent was obtained from the patients or their relatives for data analysis in full compliance with the current legislation on personal data protection.
ResultsDuring the study period, a total of 141 patients on a ≥72 h-course of invasive mechanical ventilation were admitted. Twelve patients were excluded due to pre-existing kidney failure upon admission or for developing it within the first 72 h (KDIGO ≥ 3), 1 due to hypophosphatemia, and 34 due to death within the first 72 h after admission (Fig. 1, Patient flow).

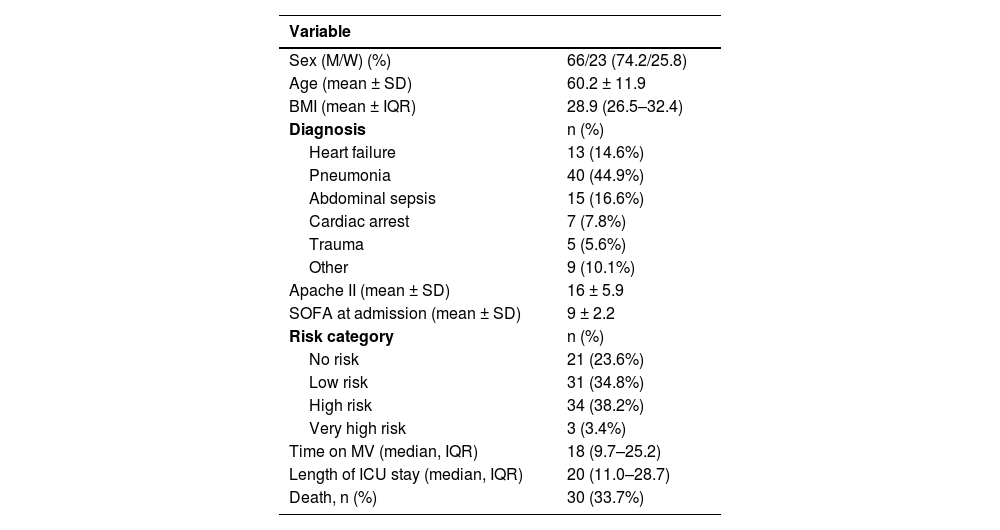
The baseline characteristics of the patient population, including their distribution in the risk categories of the consensus conference, are shown in Table 2. Among the risk factors included, the most common one was reduced food intake prior to the ICU admission (55%) followed by the use of certain drugs (35%). Unintentional weight loss and prior alcoholism, or drug abuse were each represented by one patient.
Baseline characteristisc of the patients.
| Variable | |
|---|---|
| Sex (M/W) (%) | 66/23 (74.2/25.8) |
| Age (mean ± SD) | 60.2 ± 11.9 |
| BMI (mean ± IQR) | 28.9 (26.5–32.4) |
| Diagnosis | n (%) |
| Heart failure | 13 (14.6%) |
| Pneumonia | 40 (44.9%) |
| Abdominal sepsis | 15 (16.6%) |
| Cardiac arrest | 7 (7.8%) |
| Trauma | 5 (5.6%) |
| Other | 9 (10.1%) |
| Apache II (mean ± SD) | 16 ± 5.9 |
| SOFA at admission (mean ± SD) | 9 ± 2.2 |
| Risk category | n (%) |
| No risk | 21 (23.6%) |
| Low risk | 31 (34.8%) |
| High risk | 34 (38.2%) |
| Very high risk | 3 (3.4%) |
| Time on MV (median, IQR) | 18 (9.7–25.2) |
| Length of ICU stay (median, IQR) | 20 (11.0–28.7) |
| Death, n (%) | 30 (33.7%) |
BMI, body mass index; IQR, interquartile range; MV, mechanical ventilation; SD, standard deviation.
The incidence rate of hypophosphatemia was 32.6% (29 out of 89 patients). The evolution of the levels of the different electrolytes studied (phosphate, magnesium, potassium) is shown in Fig. 2. In patients with hypophosphatemia, phosphate levels dropped from 3.57 ± 1.02 mmol/L down to 1.87 ± 0.65 mmol/L (a 52.3% drop).
. The number of observations (n) ranges from 23 to 29 for the group with hypophosphatemia, and 54–60 for the group without hypophosphatemia. Mg, magnesium; K, potassium; P, phosphate; In, mmol/L. Measurements: 1. Admission; 2. 96 h; 3. 7–10 days.")
Electrolyte evolution.
Data expressed as medians and interquartile range (IQR). The number of observations (n) ranges from 23 to 29 for the group with hypophosphatemia, and 54–60 for the group without hypophosphatemia. Mg, magnesium; K, potassium; P, phosphate; In, mmol/L. Measurements: 1. Admission; 2. 96 h; 3. 7–10 days.
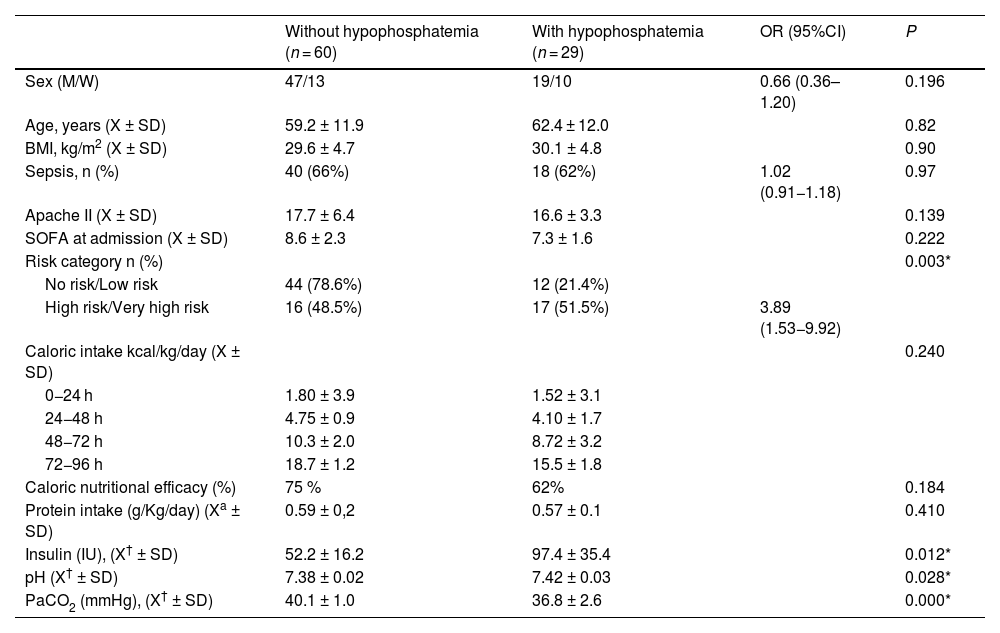
In the overall population, the mean caloric intake at 96 h was 17.4 ± 4.1 kcal/kg/24 h, and in both groups, nutritional efficiency reached 70% of the target of 25 kcal/kg of current body weight, without any differences in the rate of increase across different days (Table 3). The doses of protein administered averaged 0.58 g/kg/day across the 4 days in all patients, with no differences being reported between the groups (0.59 ± 0.2 vs 0.57 ± 0.1).
Univarte analysis. Groups based on the development, or not, of hypophosphatemia 96 h after the ICU admission.
| Without hypophosphatemia (n = 60) | With hypophosphatemia (n = 29) | OR (95%CI) | P | |
|---|---|---|---|---|
| Sex (M/W) | 47/13 | 19/10 | 0.66 (0.36–1.20) | 0.196 |
| Age, years (X ± SD) | 59.2 ± 11.9 | 62.4 ± 12.0 | 0.82 | |
| BMI, kg/m2 (X ± SD) | 29.6 ± 4.7 | 30.1 ± 4.8 | 0.90 | |
| Sepsis, n (%) | 40 (66%) | 18 (62%) | 1.02 (0.91−1.18) | 0.97 |
| Apache II (X ± SD) | 17.7 ± 6.4 | 16.6 ± 3.3 | 0.139 | |
| SOFA at admission (X ± SD) | 8.6 ± 2.3 | 7.3 ± 1.6 | 0.222 | |
| Risk category n (%) | 0.003* | |||
| No risk/Low risk | 44 (78.6%) | 12 (21.4%) | ||
| High risk/Very high risk | 16 (48.5%) | 17 (51.5%) | 3.89 (1.53−9.92) | |
| Caloric intake kcal/kg/day (X ± SD) | 0.240 | |||
| 0−24 h | 1.80 ± 3.9 | 1.52 ± 3.1 | ||
| 24−48 h | 4.75 ± 0.9 | 4.10 ± 1.7 | ||
| 48−72 h | 10.3 ± 2.0 | 8.72 ± 3.2 | ||
| 72−96 h | 18.7 ± 1.2 | 15.5 ± 1.8 | ||
| Caloric nutritional efficacy (%) | 75 % | 62% | 0.184 | |
| Protein intake (g/Kg/day) (Xa ± SD) | 0.59 ± 0,2 | 0.57 ± 0.1 | 0.410 | |
| Insulin (IU), (X† ± SD) | 52.2 ± 16.2 | 97.4 ± 35.4 | 0.012* | |
| pH (X† ± SD) | 7.38 ± 0.02 | 7.42 ± 0.03 | 0.028* | |
| PaCO2 (mmHg), (X† ± SD) | 40.1 ± 1.0 | 36.8 ± 2.6 | 0.000* |
BMI, body mass index; kcal, kilocalorie; SD, standard deviation; X, mean.
Nutritional efficacy: calories provided/calculated target.
The mean insulin doses were 71.6 IU, and the pH and PaCO2 values were 7.39 ± 0.03 and 39.0 ± 2.3 (mmHg), respectively, with a mean of 9.2 determinations. Regarding changes in acid-base status between admission and day 4, there significant changes were reported in the group with hypophosphatemia, with drops of PaCO2 from 40.3 ± 2.7 down to 36.8 ± 2.6 mmHg.
In the univariate analysis (Table 3), factors related to the occurrence of hypophosphatemia were the risk category levels (grouped as none-low and high-very high), the mean insulin doses administered, and the pH and PaCO2 values. Caloric intake, although not statistically significant, was quantitatively lower in those who developed hypophosphatemia.
In the multivariate analysis, the variables related to the development of hypophosphatemia were insulin doses (IU) and the PaCO2 values (Table 4). The variable representing risk categories was not included in the final multivariate model as it was not statistically significant.
Multivariate analysis.
| B | SD | Wald | DF | Sig. | Exp(B) | 95%CI for EXP(B) | ||
|---|---|---|---|---|---|---|---|---|
| Inferior | Superior | Inferior | Superior | Inferior | Superior | Lower | Higher | |
| Insulin (1 IU) | 0.032 | 0.009 | 12.606 | 1 | 0.000 | 1.033 | 1.014 | 1.051 |
| PaCO2 (1 mmHg) | −1.220 | 0.293 | 17.370 | 1 | 0.000 | 0.295 | 0.166 | 0.524 |
| Constant | 45.435 | 11.306 | 16.148 | 1 | 0.000 | 00.000 | ||
The main finding of the study is the high incidence rate of hypophosphatemia that occurs after several days on mechanical ventilation in patients admitted to the intensive care unit. Although it occurs more frequently in the very high-risk category, it is also possible with fewer risk factors or even none, so we believe that monitoring is mandatory in all patients who initiate invasive ventilatory support treatment. We have not yet demonstrated a relationship with the provided caloric intake, although it has been administered following the latest recommendations on nutritional support in critically ill patients, progressively within the first few days, and not exceeding 70% before 96 h.
The incidence found in our study—32.6%—falls within the middle range of what is reported in the scientic medical literature. In the systematic review by Cioffi et al.,8 the incidence rate ranged from 7% to 62%, being the subgroups of patients admitted to Intensive Care Units (ICUs) and those with nutritional caloric intake > 20 kcal/kg/day at the higher end (mean incidence of 27% with a 95%CI of 21%–34%). Differences are due to the type of study (retrospective or prospective), the type of patients studied, and the cut-off value used to define hypophosphatemia.14–18 In our case, the incidence rate may have been reduced in some high-risk patients after adjusting the nutri-metabolic treatment according to the existing protocol.
All available guidelines and consensus statements (NICE, ASPEN, Friedli) establish a series of risk factors and categorize patients in different groups.10–12 We only know of 1 study that has compared the performance of 2 of these scales (modified NICE and ASPEN). In 478 neurocritical patients with an incidence rate of 17.5%, the areas under the ROC curve were 0.568 (0.522−0.613) and 0.597 (0.551−0.641), respectively, far from being useful as predictive tools.19 A different study on the NICE scale also found poor discrimination among all diagnostic criteria (area under the ROC curve from 0.43 to 0.53) and concluded that they uncertainly predict the development of RS.20 We chose the European consensus conference (Friedli), and a recent prospective validation study of 542 patients which demonstrated a positive mortality gradient as the risk category increased.21 Although we cannot establish that relationship due to our sample size, the frequency of the 4 categories is very similar to that of this study, and the differences (between low and high) can be attributed to the fact that 2 risk factors—the estimated weight loss and days of fasting, or low pre-admission intake—are subject to the subjectivity of the person taking the patient’s medical history.
We did not find a correlation with the caloric intake administered within the first 96 h since admission. Since enteral nutrition started, on average, 24 h after admission, the mean was calculated with a 3-day intake. Since the protocol for initiating enteral nutrition in both centers includes a progressive increase within the first 7 days to reach the caloric target of 25 kcal/kg/day, the mean intake remained at 17 kcal/kg/day on day 4, somewhat higher than advised (10–15 kcal/kg/day) in guidelines for preventing the RS, but far from the intakes suggested by other groups where an association was found. For instance, in the recent Nutrirea-3 clinical trial, the reported incidence rate of hypophosphatemia is higher and statistically significant in the standard caloric intake group (25 kcal/kg) vs the low-calorie intake group (6 kcal/kg) (61.3% vs 53.6%). However, the authors themselves comment in the discussion that these differences had no impact on the levels of other electrolytes (potassium, magnesium) or mortality, so they question their clinical relevance.22
Recently, there have been reports of the potential protective, or harmful role of proteins in the genesis of the RS. In a group of critically ill patients with COVID-19-induced pneumonia, Vahdat et al.13 found that for every gram of protein provided, the likelihood of developing the RS dropped by 90%. On the other hand, Slingerland-Boot et al.23 described that higher protein intake in patients with hypophosphatemia within the first 3 days following the ICU admission is associated with higher mortality at 6 months.
The fact that we did not find a relationship with caloric intake at a time when it is generally recommended to be administered progressively with a target of 70% by the 4th day of admission24 makes us reconsider the most common cause of hypophosphatemia in critically ill patients and its designation.25 While the existence of potential hypophosphatemia in these patients is indisputable, its origin may be linked to other causes. Hypophosphatemia at the ICU setting results from phosphate redistribution and renal losses.26 Glucose-insulin therapy, respiratory alkalosis, and catecholamines can cause hypophosphatemia related to cellular redistribution (from extracellular to intracellular). Hypophosphatemia due to renal losses occurs due to diuretics, corticosteroids, and continuous renal replacement therapy (CRRT).27
We studied 2 of these factors—the administration of insulin and acid-base status. Regarding insulin doses, a significant difference between the groups was reported, with nearly twice as many units administered in the group with hypophosphatemia. Most patients who received insulin (60%) had diabetes and required it prior to admission. However, a significant percentage was associated with the metabolic response to the critical condition. The pathophysiological mechanism of the redistribution of phosphate from the extracellular to the intracellular space is well-known.28 Insulin, whether administered exogenously or secreted as a result of carbohydrate intake, increases the cellular uptake of phosphate and other ions (potassium, magnesium), triggering drops in plasma levels. Inside the cell, phosphate is primarily used for energy production in the form of adenosine triphosphate (ATP). In the case of the acid-base status, and since all patients were on mechanical ventilation, we should mention that unintentional hyperventilation can occur (there were no patients with traumatic brain injury in our sample), leading to respiratory alkalosis. This causes an increase in intracellular pH, resulting in an increased activity of the enzyme phosphofructokinase and glycolysis, triggering an increased demand for intracellular phosphate and a corresponding decrease in the extracellular (plasma) space.29 We should mention that it is not necessary to reach alkaline levels in plasma, but rather significant changes in the acid-base status (alkalosis), as observed in our sample.
The limitations of this study are the following ones. Despite being a prospective study, the limited sample size prevented us from obtaining conclusive results regarding the relationships between hypophosphatemia and caloric intake, as we couldn’t analyze the multiple interactions among the associated variables. Also, we could not include in the analysis several alternative causes of hypophosphatemia that are commonly found in these patients (certain drugs such as corticosteroids, diuretics, etc.). We were also unable to analyze clinical outcomes in terms of morbidity and mortality associated with the development of hypophosphatemia and whether these outcomes can be modified by treating hypophosphatemia. This is a controversial issue for which there is still not enough scientific evidence.30,31 The relationship between hypophosphatemia and the development of organ dysfunction in patients with already severe underlying conditions is highly debatable. Also, it would be ethically challenging not to provide phosphate supplementations to patients with levels below average. In our case, all diagnosed patients received IV phosphate according to a predefined protocol. Nonetheless, the strength of this study is that it is one of the series with the largest number of critically ill patients on mechanical ventilation reported to this date. Also, we believe the focus should be on detecting and treating hypophosphatemia rather than practicing caloric restriction in a specific subgroup of patients.32 We suggest that plasma phosphate levels should be monitored in all patients after starting invasive mechanical ventilation, especially in those who require insulin for glycemic control, or present with respiratory alkalosis.
ConclusionsThe incidence rate of hypophosphatemia in critically ill patients on invasive mechanical ventilation is high and cannot be predicted by the risk categories of developing the RS. Therefore, routine monitoring of phosphate levels should be considered. In our patient sample of normal phosphate levels upon admission, hypophosphatemia is related to insulin doses and the degree of ventilation (PaCO2) rather than the reduced caloric intake administered.
Authors’ contributionsStudy design: Manuel Colmenero. Francisco Manzano
Data mining: Rocio Morón, Purificación Fernández, Inmaculada de Dios, María Reyes Mañas Vera.
Result analysis: Manuel Colmenero, Rocío Morón, Francisco Manzano
Manuscript draftint: Manuel Colmenero, Francisco Manzano
Manuscript review: Rocío Morón, Purificación Fernández, Inmaculada de Dios, María Reyes Mañas Vera.
FundingNone declared.
Conflicts of interestNone declared.

