










To study the organization of inter-hospital transport of pediatric and neonatal patients in Spain, Portugal and Latin America.
DesignAn observational study was performed. An on-line survey was sent by email including questions about characteristics of national, regional and local health transport systems, vehicles, material, and composition of the transport team and their training.
SettingHospital pediatric healthcare professionals treating children in Spain, Portugal and Latin America.
ResultsA total of 117 surveys from 15 countries were analyzed. Of them, 55 (47%) come from 15 regions of Spain and the rest from Portugal and 13 Latin American countries. The inter-hospital transport of pediatric patients is unified only in the Spanish regions of Baleares and Cataluña and in Portugal. Chile has a mixed unified transport system for pediatric and adult patients. Only 51.4% of responders have an educational program for the transport personnel, and only in 36.4% of them the educational program is specific for pediatric patients. In Spain and Portugal the transport is executed mostly by public entities, while in Latin America public and private systems coexist. Specific pediatric equipment is more frequent in the transport teams in the Iberian Peninsula than in Latin American teams. The specific pediatric transport training is less frequent for teams in Latin America than on Spain and Portugal.
ConclusionsThere is a great variation in the organization of children transport in each country and region. Most of countries and cities do not have unified and specific teams of pediatric transport, with pediatric qualified personnel and specific material.
Estudiar la organización del transporte interhospitalario pediátrico y neonatal en la península ibérica y Latinoamérica.
DiseñoEstudio observacional prospectivo mediante una encuesta enviada por correo electrónico con preguntas sobre el sistema de transporte nacional, regional y local, el tipo y vehículo de traslado, el material y el personal y su formación.
ÁmbitoResponsables pediátricos de hospitales de España, Portugal y Latinoamérica.
ResultadosSe analizaron 117 encuestas provenientes de 15 países. De ellas, 55 (47%) procedían de 15 comunidades autónomas de España y el resto de Portugal y de 13 países latinoamericanos. Muy pocas regiones y ciudades tienen un sistema de transporte pediátrico y neonatal específico. El transporte solo está unificado en las comunidades españolas de Baleares y Cataluña y en Portugal. En Chile el sistema de transporte es mixto, pediátrico y del adulto. Solo un 51,4% de los hospitales tiene un sistema de formación del personal de transporte, y solo en el 36,4% la formación es específica en transporte pediátrico. En España y Portugal los sistemas de transporte son fundamentalmente públicos, mientras que en Latinoamérica coexisten sistemas públicos y privados. Los equipos de transporte de la península ibérica tienen más material pediátrico y neonatal y reciben más formación en transporte pediátrico que los de Latinoamérica.
ConclusionesExiste una gran variabilidad en la organización del transporte pediátrico en cada país y región. En la mayoría de los países y ciudades no existe un sistema unificado y específico de transporte pediátrico con un personal cualificado y un material de traslado específico.
Medical transport takes human and material medical care resources to places that lack such resources, and in turn takes the ill patient to the place where medical care resources are available–this being particularly important when intensive care or emergency surgery is needed.1,2
Medical transport is of vital importance within the chain of care. Although speed is clearly an important factor in the emergency transfer of patients, the quality of transport is crucial–and this fundamentally depends on the organization, coordination and preparation of the transport system and equipment, and on the material means available.1,2
There are different types of medical transport. Depending on the means used, it can be classified as overland, by air, or by water (maritime-fluvial). Overland transport is the most widely used modality in view of its accessibility and operability. In turn, depending on where it takes place, transport is classified as out-hospital, i.e., from the site of the emergency to the healthcare center; inter-hospital; or in-hospital.
Pediatric transport is a key element in the chain of survival in critically ill children and for the provision of healthcare continuity.1 The importance of organizing a pediatric system differentiated from adult transport is due to the specific characteristics of pediatric patients, which have their own specific physiological and disease parameters. Furthermore, pediatric transfer often requires the use of materials and treatment techniques different from those used in adults–and this in turn implies the need for specific training on the part of the staff in charge of transport.1,3
Despite its importance, no large multicenter studies have analyzed the characteristics and needs of pediatric transport–such information being essential in order to plan and organize a transport system for this particular population group.
The present study analyzes and compares the organization of inter-hospital pediatric and neonatal transport in Spain, Portugal and Latin America.
MethodsA prospective observational study was carried out based on a survey distributed by e-mail among pediatric care supervisors belonging to hospitals and transport systems in Spain, Portugal and Latin America. An invitation to participate was also sent through the Spanish Society of Pediatric Intensive Care (Sociedad Española de Cuidados Intensivos Pediátricos [SECIP]) and the Latin American Society of Pediatric Intensive Care (Sociedad Latinoamericana de Cuidados Intensivos Pediátricos [SLACIP]).
The survey was structured into three levels: national, regional and local transport (i.e., in the town or city where the hospital is located). The following variables were collected for each level: type of system (unified, neonatal, pediatric or mixed; public or private); care period, the existence or not of a coordinating center, and location.
In addition, an analysis was made of the following characteristics of each hospital included in the study: pediatric population covered; age range of the attended patients; number of children and neonates transported annually; the most frequent pediatric and neonatal disorders requiring transport; transport system used; type of patients; vehicles used for transfer (overland, by air, or by water/maritime-fluvial); pediatric and neonatal transfer material, transfer team and training; and the documentation generated during patient transfer. The survey can be consulted in Appendix B.
The data were processed using the SPSS version 20.0 statistical package (IBM, Armonk, NY, USA). The comparison of frequencies was based on the chi-squared test or Fisher test, according to the number of responses. The Student's t-test was used for the comparison of continuous variables. Statistical significance was considered for p<0.05.
ResultsA total of 117 surveys from 15 countries were analyzed. Fifty-five of these surveys (47%) came from Spanish hospitals (in 15 of the 17 autonomous communities in the country), while the remaining surveys came from 62 hospitals in 13 Latin American countries (Chile, Argentina, Mexico, Colombia, Honduras, Dominican Republic, Brazil, Guatemala, Ecuador, Paraguay, Peru, Costa Rica and Venezuela) and Portugal.
A total of 89.7% of the hospitals are receptors of pediatric patient transport, and 91.3% are the issuers of such transport. In turn, 5.9% of the hospitals have a Pediatric Intensive Care Unit (PICU) only; 11.8% have a Neonatal Intensive Care Unit only; and 70.6% have both Units.
Characteristics of the transport systemThe general characteristics of national, regional and local transport are summarized in Table 1.
General characteristics of the national, regional and local medical transport system.
| Type of transport | National (%) | Regional (%) | Local (%) |
|---|---|---|---|
| Unified system | 10.6 | 39.1 | 40 |
| Coordinating center | 76.9 | 93 | 84 |
| Public system | 83 | 88.6 | 78.3 |
| Public and private | 16.7 | 9.1 | 13 |
| Private | 0 | 2.3 | 8.7 |
| 24-Hour availability | 100 | 100 | 100 |
| Pediatric only | – | 4.5 | 2.2 |
| Neonatal only | – | 25 | 10.9 |
| Pediatric and neonatal | – | 6.8 | 8.7 |
| Pediatric and adult | – | 63.6 | 78.3 |
All of the hospitals have a pre-hospital medical care system established at national level.
Only two countries have a unified national transport system. Portugal possesses a unified inter-hospital system specifically designed for pediatric and neonatal patient transport. This is a public system with 24-hour availability, and is organized into three regional areas (North, Center and South)–each with its own coordination system.
Chile has a mixed (pediatric and adult) unified public medical transport system organized by the Emergency Care System (Sistema de Atención Médica de Urgencia [SAMU]). Transport is available 24hours a day, and there is a specific local coordinating center per region–with a regional regulating center and bases distributed throughout the different towns that in turn are regulated nationally by the Ministry of Health. The staff is not specialized in pediatric care but must complete a pediatric transportation course.
Other countries such as Spain do not have a unified national medical transport system. A specific pediatric unified transport system is found in only two Autonomous Communities (Catalonia and the Balearic Islands). The rest of the Communities have a mixed unified system for adults and children, and some Communities such as Madrid offer specific neonatal transport.
The rest of the Latin American countries have no unified transport system: public and private systems that are not of a specifically pediatric nature are seen to coexist.
The characteristics of the patients, transport means, teams and training are shown in Table 2.
Characteristics of the patients, transport means, staff and training.
| Characteristics | |
| Age of the transported children | |
| 0–14 years | 64.8 |
| 0–18 years | 18.9 |
| Several ranges | 16.3 |
| Causes of pediatric transfer | |
| Respiratory problems | 36 |
| Cardiac problems | 19.1 |
| Traumatisms | 18 |
| Others | 26.9 |
| Causes of neonatal transfer | |
| Prematurity | 42.9 |
| Congenital heart diseases | 18.4 |
| Meconial aspiration syndrome | 6.1 |
| Others | 32.5 |
| Overland transport | |
| Non-medicalized conventional ambulance | 61.9 |
| Mobile ICU | 67.5 |
| Mobile PICU | 27.2 |
| Air transport | |
| Medicalized helicopter | 46.9 |
| Aircraft ambulance | 22.1 |
| Conventional aircraft | 13.3 |
| Water (maritime-fluvial) | 0 |
| Transport team | |
| Team belonging to the hospital | 17 |
| Public transport team | 25.9 |
| Private transport team | 8.9 |
| Combination of several systems | 18.8 |
| No specific transport | 26.8 |
| Transport staff | |
| Specific of pediatric transport (physician and nurse) | 6.3 |
| Staff of the PICU | 8.3 |
| Emergency care services | 13.5 |
| Staff belonging to the issuing hospital | 9.4 |
| Paramedics | 3.1 |
| Different combinations | 59.4 |
| Staff training | |
| Transport staff training system | 51.4 |
| Specific training in pediatric transport | 36.4 |
Data expressed as percentages.
In most cases transport team training is not structured: there are variations in its theoretical and practical dimensions, organization by the Department of Emergency Care or the PICU, and in the frequency of training.
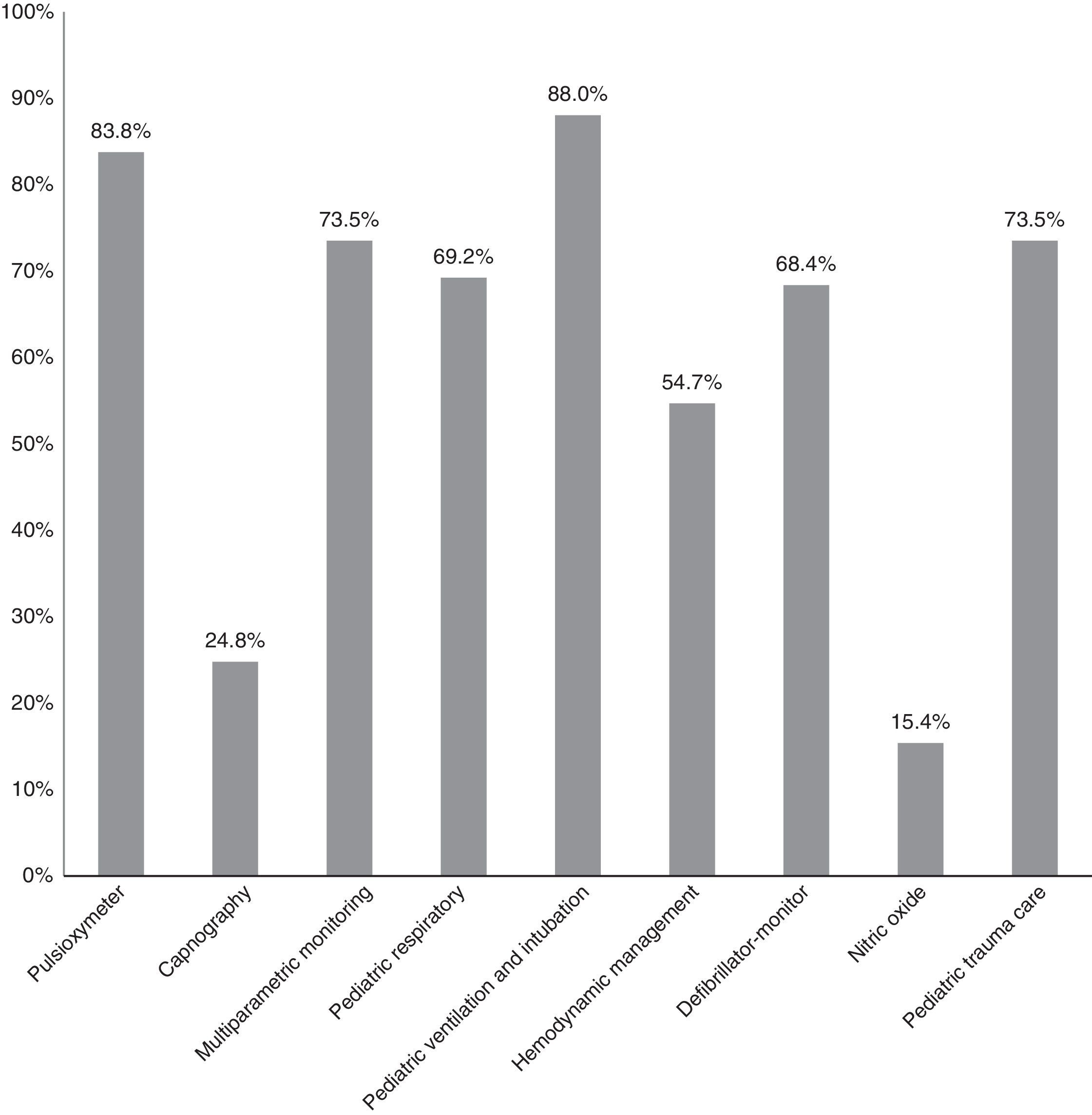
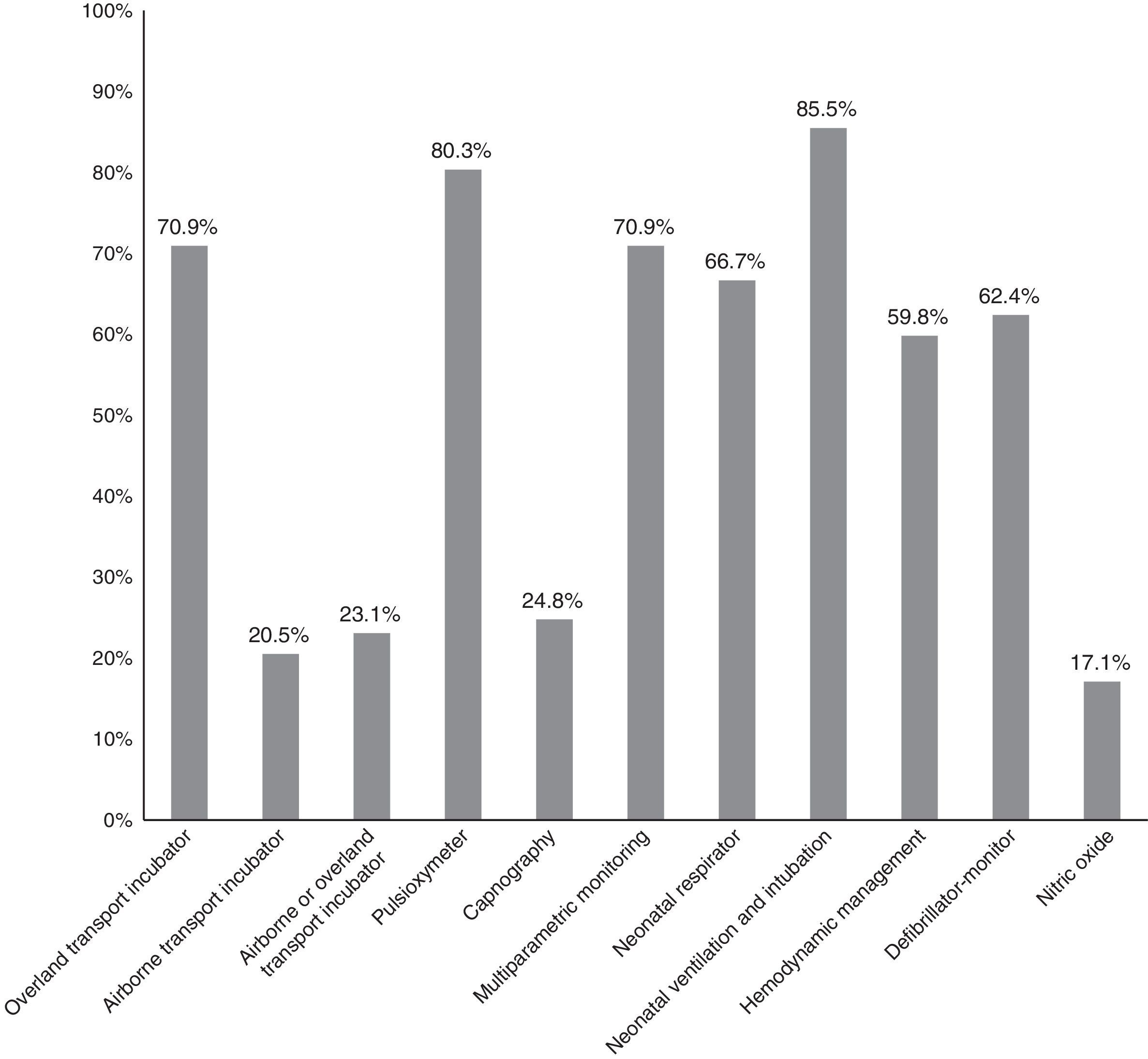
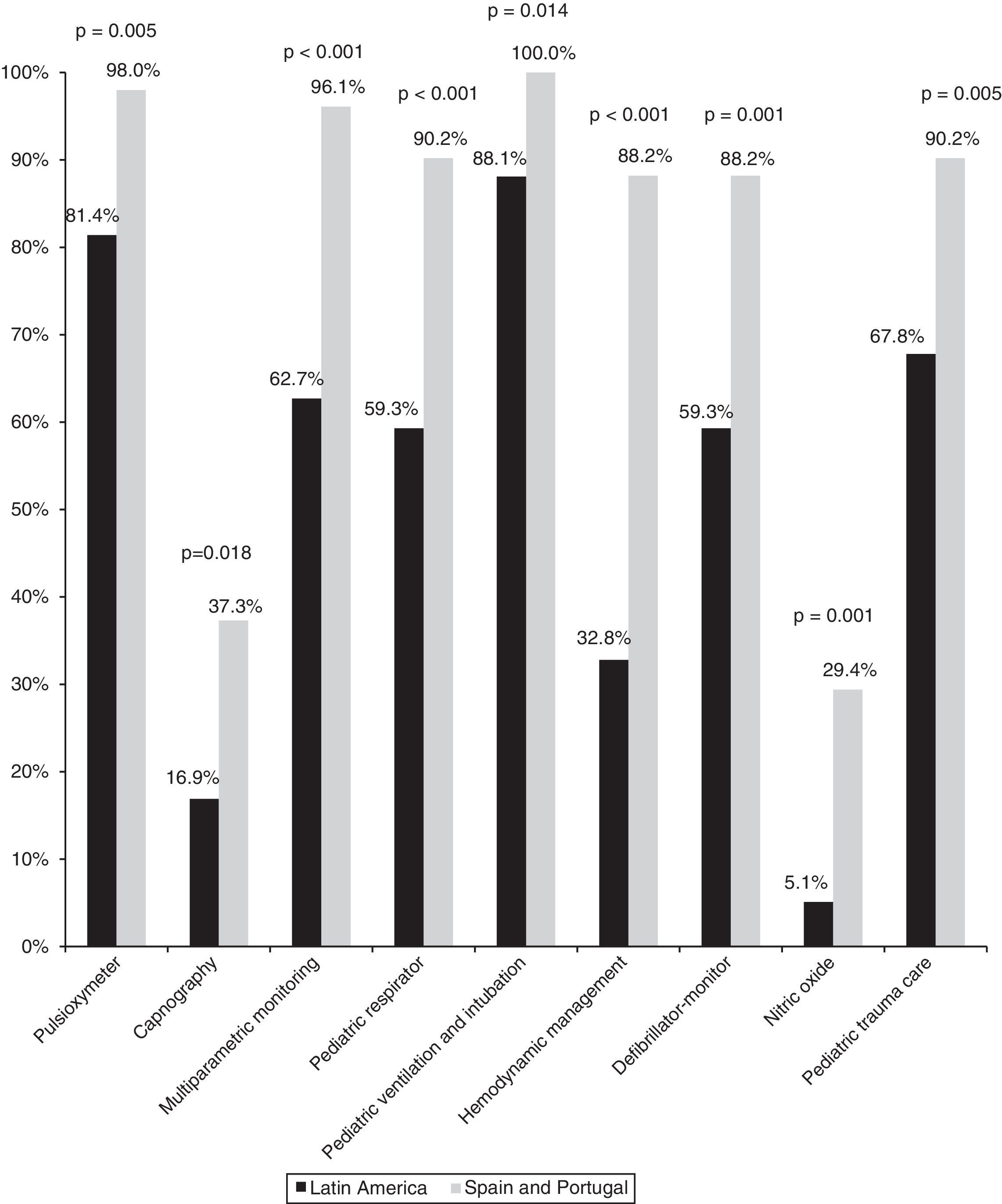
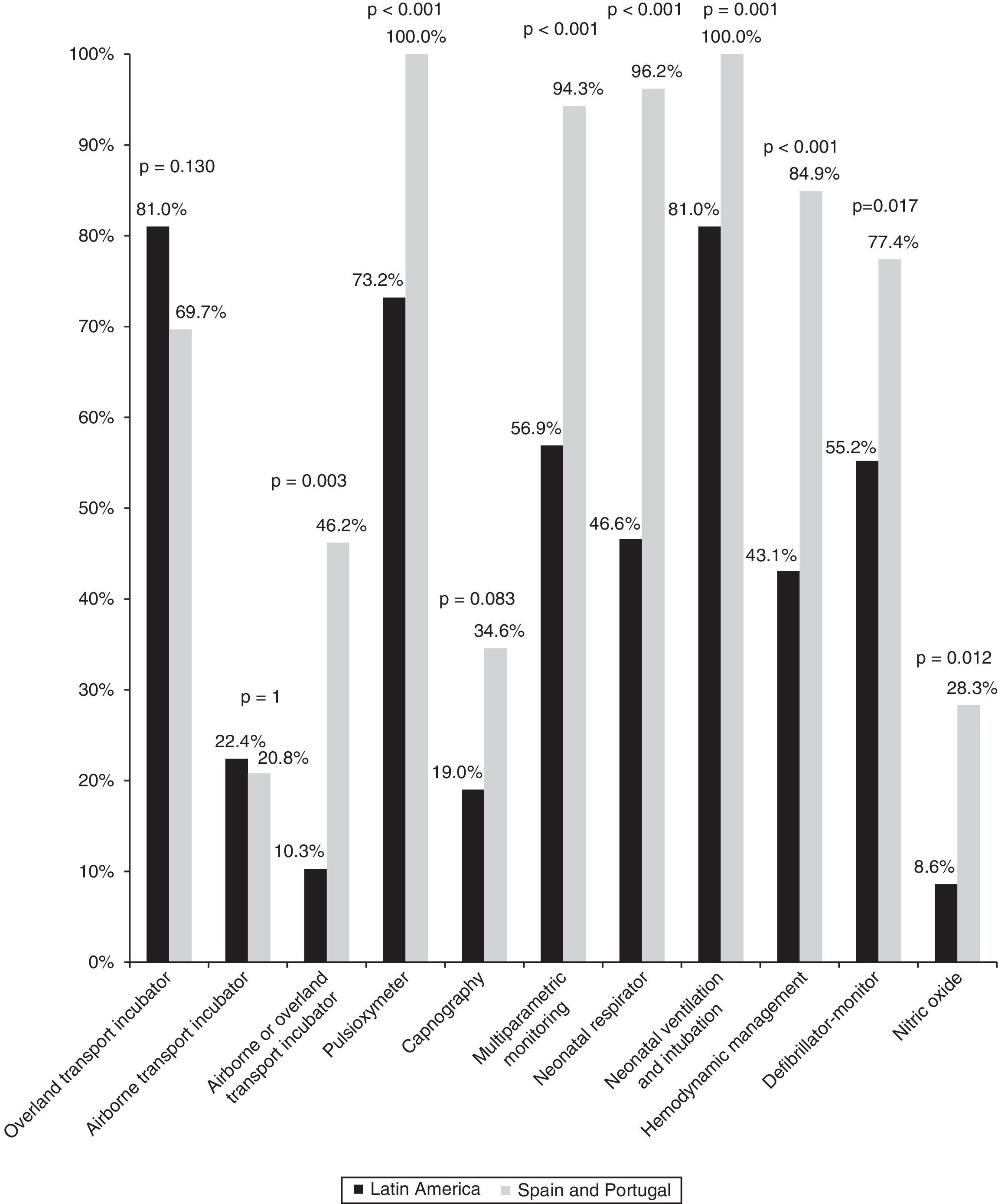
The available neonatal and pediatric transport material is described in Figs. 1 and 2.
Regarding the generated documentation, all of the hospitals make use of a specific form containing the data referred to transfer (patient information, treatments, evolution, etc.), and 58.8% require written informed consent.
Assessment of the transport systemOnly 17 of the 117 surveys (14.5%) assessed the transport system. Of these, 11.8% consider the transport system in their locality to be adequate; 23.5% consider it to be sufficient; and 64.7% believe transport is insufficient and needs to be improved.
Comparison between the Iberian Peninsula and Latin AmericaTable 3 summarizes the comparison of the different transport systems between the Iberian Peninsula and Latin America.
Comparison of transport between Latin America and Spain and Portugal.
| Latin America (%) | Spain and Portugal (%) | p-value | |
|---|---|---|---|
| Unified regional transport | 26.7 | 52.7 | 0.007 |
| Unified local transport | 35.5 | 45.3 | 0.341 |
| Type of system | 0.017 | ||
| Pediatric | 4.8 | 0 | |
| Neonatal | 0 | 20 | |
| Pediatric and neonatal | 0 | 16 | |
| Pediatric and adult | 95.2 | 64 | |
| Public transport | 73.3 | 96.6 | 0.002 |
| 24-Hour availability | 100 | 100 | 0.467 |
| Coordinating center | 62.6 | 77.3 | 0.185 |
| Transport team | 0.001 | ||
| Specific public | 10.3 | 42.6 | |
| Specific of the hospital | 13.8 | 20.4 | |
| Specific private | 13.8 | 3.7 | |
| Non-specific | 36.2 | 16.7 | |
| Others | 1.7 | 3.7 | |
| Several of the above | 24.1 | 13 | |
| Transport training | 29.8 | 76 | 0.001 |
| Pediatric transport training | 19.6 | 54.2 | 0.001 |
Medical transport is more unified in Spain and Portugal, and is more often of public and specifically pediatric or neonatal compared with Latin America.
Transport meansThe use of mobile ICUs and medicalized helicopters as transport means is more common on the Iberian Peninsula, while in Latin America conventional ambulances and aircraft ambulances mark the tendency (Fig. 3).
Transport material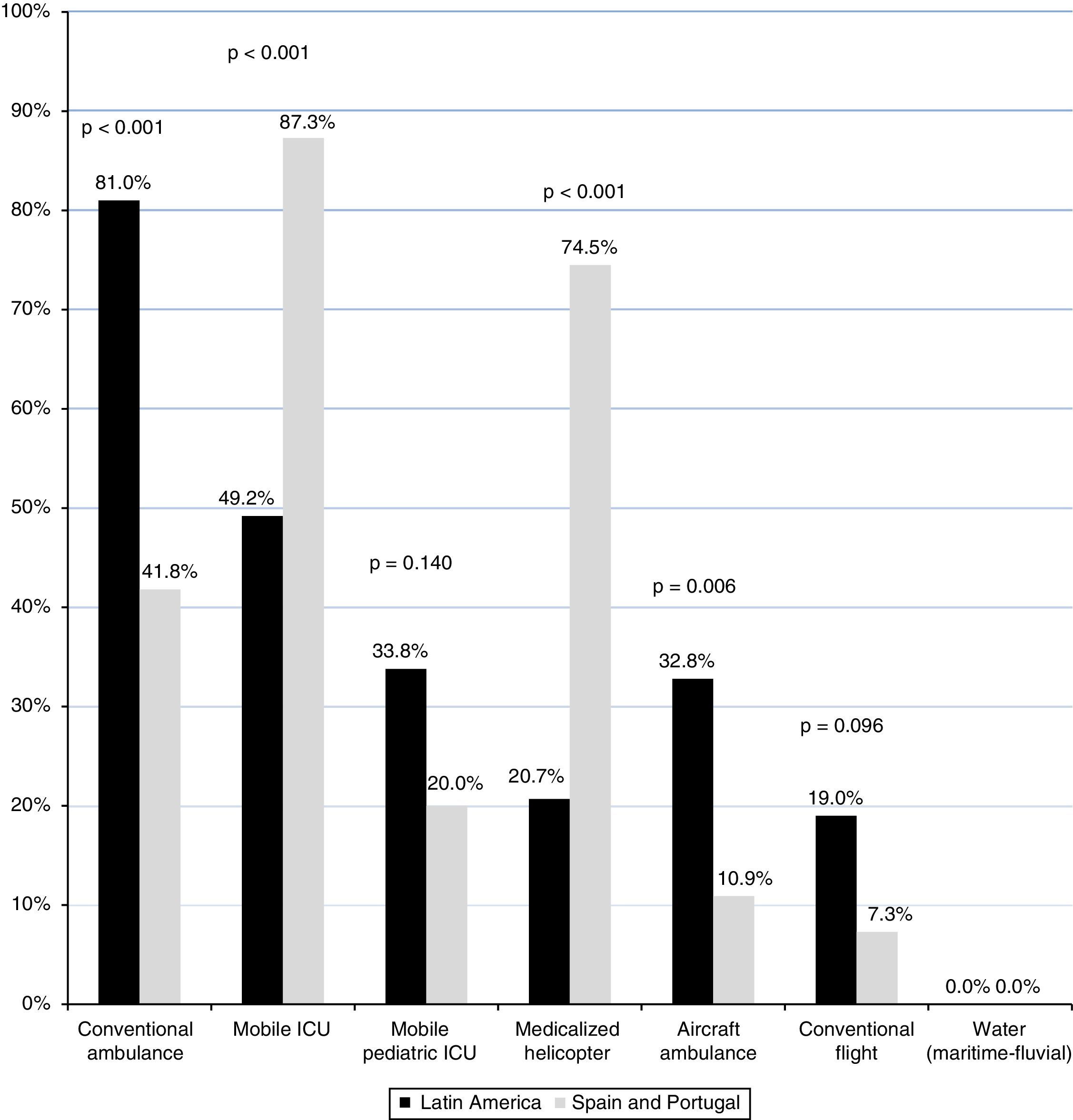
On the Iberian Peninsula, the teams have a greater availability of transport material–both pediatric and neonatal–than in Latin America (Figs. 4 and 5).
A specific pediatric training system for the medical transport staff is more frequently found in Portugal and Spain than in Latin America (Table 3 and Fig. 6).
Discussion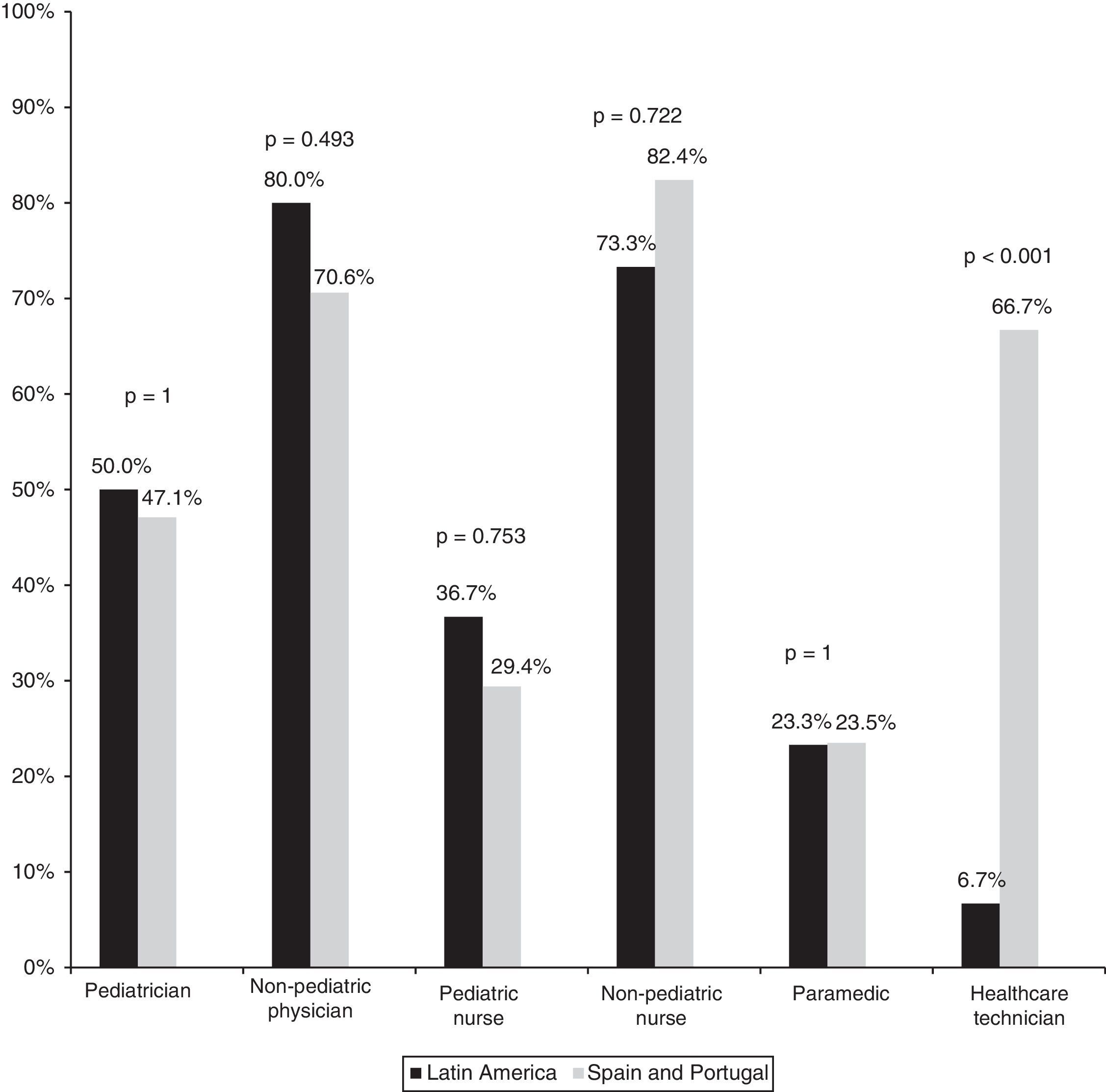
This is the first international multicenter study including data from 15 countries to analyze the characteristics of inter-hospital pediatric transport.
Pediatric transport is a high-risk situation and so must be carried out by adequately trained staff with material resources adapted to the size, age and characteristics of the patient. Several authors have demonstrated the importance of creating medical transport teams specialized in pediatric patients, with nursing staff trained in the care of pediatric and neonatal patients.1,3 It has been shown that although transport carried out by teams with these characteristics may imply longer response times, the outcomes are better in terms of clinical evolution and survival, with fewer adverse events.1,3–5
General characteristics of transportOur results show that at present, most of the surveyed countries do not have a unified pediatric transport system, and most children are transferred by non-pediatric teams. The coexistence of different models–public and private, pediatric and adult, neonatal or pediatric, local and regional–within one same area is relatively common, and this makes the optimization of human and material resources difficult. Only Portugal, Catalonia and the Balearic Islands have a unified specific pediatric transport system, and these are precisely the only areas that hold a positive view of the system.6–8 On the other hand, the training of medical transport staff is generally inadequate. Very few hospitals have transport training programs, and many teams do not have specific pediatric training.
Little information is available on the organization of medical transport in other countries. In relation to adults, The Netherlands, United Kingdom, Australia and New Zealand expect all hospitals to be able to transport critical patients by means of their own specialized staff.4 In the United States, the composition of the teams is not homogeneous, and in many hospitals the teams are composed of a nurse, a paramedic and a driver–though some teams are highly trained.4 In Canada, many critical patient transport teams also operate without a physician. However, the paramedics are well trained and are experienced in emergencies and the transfer of critical patients.4
It is very difficult to establish teams specialized in the transport of pediatric patients in all hospitals. The most reasonable solution therefore might be to organize a coordinating center at regional or local level, with specifically pediatric and neonatal transport teams dependent upon some of the receptor hospital centers in the region–as successfully occurs in Portugal, Catalonia and the Balearic Islands.6–8
Furthermore, it is important to note that only 67.5% of the teams are equipped with a mobile ICU, and only 27.7% have a mobile ICU adapted to pediatric patients–despite the studies that show transport under the best possible conditions to lessen the incidence of adverse events (medical or technical).9,10 Technical incidents represent up to 46% of the total,4 which underscores the importance of adequate knowledge of the equipment used.9,10
In coincidence with other studies,10 the disorders most often requiring transport are of a respiratory, cardiac and traumatic nature, together with specifically pediatric conditions such as prematurity, congenital heart disease or meconial aspiration syndrome. These circumstances in turn require specific knowledge and practical experience. Consequently, specific theoretical and practical staff training is a crucial aspect of medical transport, along with the availability of clinical guides as support for the diagnosis, management and transfer of critical patients.11,12
Comparison between the Iberian Peninsula and Latin AmericaMedical transport on the Iberian Peninsula is generally public, is more often unified, and has more specific pediatric and neonatal transport teams, which moreover receive greater training in patient transport. With regard to the material resources on the Peninsula, the use of a mobile ICU as means of transport is more common, and the teams have more both pediatric and neonatal care material than in Latin America. These imbalances are probably due in part to economic differences between countries, though health system organization capacity and awareness of medical transport as an important healthcare and social need also exert an influence.13 The existing differences are further accentuated by the greater need for pediatric transport in Latin America, where there are generally greater contrasts in healthcare coverage between the different hospitals, and the geographical distances are moreover greater.
National and international collaboration is very important to overcome these differences. Although there is some experience in pediatric transport training through the collaboration of expert teams such as for example in Honduras, a multinational work network is needed. In this sense, the creation of a Latin American Pediatric Transport Network (Red Iberoamericana de Transporte Pediátrica [RITRANSPED]) has been proposed as a means to coordinate the efforts of the different countries.
Study limitationsOur study has several limitations. Firstly, the data were obtained from an open survey, with a non-homogeneous geographical distribution of the hospitals included in the study, and we received a larger number of completed surveys from certain regions generally corresponding to the most populated cities. Because of this, the study might not exactly reflect the situation of pediatric transport, particularly in Latin America, where there is an enormous pediatric population and healthcare organization is highly diverse. On the other hand, the number of surveys returned from each country was not enough to allow comparisons by countries. In this regard, our study only analyzes a small sample not fully representative of the real situation in Latin America; the statistical conclusions are therefore of limited validity. Nevertheless, our results are useful in illustrating the main characteristics and shortcomings of the pediatric transport systems.
In contrast to the above, the number of responding centers in Spain was very high (54 hospitals), and this means that the results obtained reliably reflect the situation of pediatric transport in this country. Information was only lacking from certain Communities such as the Canary Islands, La Rioja and the cities of Ceuta and Melilla.
On the other hand, our study only addresses the general characteristics of the pediatric transport system. The creation of a clinical pediatric transport registry is needed at national and international level in order to assess the problems and requirements of transport, and to facilitate its organization and efficacy.
Lastly, the survey does not analyze the in-hospital transfer systems, which are also of great clinical relevance.14
ConclusionIn conclusion, there is great variability in the organization of pediatric transport in each country and region of the Iberian Peninsula and Latin America. In most settings, there is no unified and specific pediatric transport system, with qualified and trained staff, or with specific transfer material resources. In general, medical transport on the Iberian Peninsula is more often unified, with more specific pediatric and neonatal transport teams, and these moreover receive greater training in patient transport and have more material resources than in Latin America.
Our data may serve as a basis for further prospective studies and the drafting of recommendations referred to transport system organization at national and international level. It is the responsibility of the government authorities to ensure the design and organization of a unified pediatric transport system including the necessary transfer material resources, specific pediatric transport teams, and a well-structured staff training program.
AuthorshipSara de la Mata, María Escobar, María Cabrerizo, Marta Gómez: data collection, analysis and interpretation; drafting of the study.
Rafael González: study design; data analysis and interpretation; drafting of the study.
Jesús López-Herce Cid: study design; data analysis and interpretation; drafting of the study; study supervision and coordination.
Investigators of the Pediatric Transport Study Group: Boris Brandstrup Azuero, Jimena Del Castillo, Pedro Domínguez Sampedro, Sarah Fernández Lafever, Rafael González, Jorge López González, Maria José Solana García, Javier Urbano Villaescusa: study design; study diffusion; data interpretation.
Conflicts of interestThe authors declare that they have no conflicts of interest.
Thanks are due to the Pediatric Transport Study Group of the Sociedad Española de Cuidados Intensivos Pediátricos for its collaboration in carrying out this study.
Boris Brandstrup Azuero, María Cabrerizo Ortiz, Ángel Carrillo, Sara de la Mata Navazo, Jimena del Castillo, Pedro Domínguez Sampedro, María Escobar Castellanos, Sarah Fernández Lafever, Marta Gómez García, Rafael González, Jorge López González, Jesús López-Herce Cid, María José Solana García, Javier Urbano Villaescusa.
The following are Supplementary data to this article:

Please cite this article as: de la Mata S, Escobar M, Cabrerizo M, Gómez M, González R, López-Herce Cid J, et al. Transporte pediátrico y neonatal en España, Portugal y Latinoamérica. 2017;41:143–152.

