

The clinical value of routine chest X-rays in critical care has been questioned, but has not been studied in the trauma environment to date. The objective of this study was to identify easy to use clinical predictors of utility in this setting.
Material and methodsA prospective observational study was made in an 8-bed traumatology ICU. Severe trauma patients (ISS>15), aged 15 years or older and admitted for 48h or longer were included. Pregnant women and radiographs obtained during initial care or for reasons other than routine indication were excluded. A staff physician, separated from clinical duties, independently reviewed the films in search of changes, as described in a closed checklist. Following closed criteria, the attending physicians reported previous day clinical events and changes in clinical management after chest X-ray obtainment. Demographic and epidemiological data were also recorded. The associations among variables were studied by univariate and multivariate analysis.
ResultsA total of 1440 routine chest X-rays were obtained from 138 consecutive patients during one year. Young males prevailed (82%; 39±16 years). The most common process was severe blunt trauma (97%). Fifty-two percent suffered severe chest trauma. The mean length of stay was 12.9±10.1 days. Mechanical ventilation was used in 86.8% of the cases. A median of 10.4±9.3 films was obtained from each patient. A total of 14% of the X-rays showed changes, most commonly malpositioning of an indwelling device (6.8%) or infiltrates (4.9%). Those findings led to a change in care in 84.6% of the cases. Multivariate analysis identified the following significant (p<0.05) risk factors for radiographic changes: first two days of evolution, mechanical ventilation, worsening of PaO2/FiO2, worsening of lung compliance and changes in respiratory secretions.
ConclusionsBased on the results obtained, the risk of not identifying dangerous conditions by restricting routine chest X-rays prescription to the described conditions is low. Observing this policy would probably mean substantial savings and a reduction in radiation exposure.
El valor de la radiografía torácica rutinaria está en cuestión. Sin embargo, este asunto no ha sido suficientemente evaluado en el caso concreto del paciente traumatizado. Nos propusimos encontrar predictores de utilidad en este entorno.
Material y métodosEstudio observacional prospectivo en una UCI de traumatología de 8 camas. Se incluyeron los pacientes de más de 15 años, con traumatismo grave (ISS>15), ingresados 48h o más. Se excluyeron las mujeres embarazadas y las radiografías no rutinarias. Un miembro del equipo médico examinó de manera independiente las placas, en busca de hallazgos radiográficos según se definían en una lista cerrada. Durante la ronda diaria, los médicos al cargo comunicaron cuantos cambios en el estado clínico y en el manejo ocurrieron tras la toma de la radiografía, también siguiendo una lista de criterios cerrados. La relación entre ambas variables se estudió por análisis univariante y multivariante.
ResultadosDurante un año se obtuvieron 1.440 radiografías de 138 pacientes consecutivos. Predominaron los varones (82%), de edad joven (39±1 años). El 97% sufrieron traumatismo contuso; el 52%, traumatismo torácico grave. La estancia media se prolongó 12,9±10,1 días. En el 86,8% se empleó ventilación mecánica. De cada paciente se realizaron 10,4±9,3 placas. En el 14% hubo hallazgos relevantes, con mayor frecuencia una malposición de un dispositivo (6,8%) o infiltrados (4,9%), desencadenando una acción clínica en el 84,6% de los casos. Por análisis multivariante, se encontraron los siguientes factores de riesgo significativos (p<0,05) para un hallazgo radiográfico: primeros 2 días de evolución, ventilación mecánica, empeoramiento de la PaO2/FiO2, empeoramiento de la distensibilidad pulmonar y variación en las secreciones respiratorias.
ConclusiónDe acuerdo con estos datos, existe un riesgo pequeño de pasar por alto condiciones peligrosas si se restringe el uso de las radiografías rutinarias a las situaciones predictivas descritas. El observar esta política probablemente significaría un sustancial ahorro económico y de la emisión de radiaciones.
Routine chest X-rays (RXR) are the X-rays obtained in the critical patient in a programmed manner–generally at the start of the daily work shift–with no prior clinical indication other than the fact of being admitted to the Intensive Care Unit (ICU). This practice may be regarded as similar to the screening protocols applied in anticipation of possible serious conditions in the critical patient, such as pneumothorax, atelectasis, effusions, or other problems.1 Although RXR represent a common resource, their validity has been questioned by a growing number of authors. Indeed, following the results of several recent studies, some centers have eliminated the practice of RXR. However, there are no studies on this subject in the concrete setting of a traumatology ICU.
A number of hazards or drawbacks have been associated with RXR, including the quality shortcomings of portable X-ray devices that do not guarantee adequate image quality under the conditions found in critical patients,2 with the resulting possibility of over- or underdiagnosing important disease processes, the risk of mobilizing unstable patients, cost issues, and, finally, radiation exposure of the patient and surroundings. Based on these considerations, a number of studies have been carried out, though without firm conclusions. Nevertheless, the expert panel of the American College of Radiology recommends RXR in patients with acute cardiopulmonary diseases or subjected to mechanical ventilation,3 i.e., under circumstances that can be found in most critical patients at any given time.
The strategies of RXR versus X-rays only upon demand need not be antagonistic, but rather should be complementary. The aim of the present study was to identify predictive factors of the usefulness of RXR.
Material and MethodsA prospective observational study was conducted during 12 months in the Emergencies and Traumatology ICU of Doce de Octubre University Hospital (Madrid, Spain). This tertiary public hospital center has about 1400 beds (with 8 in this ICU), and its recruitment population corresponds to the southern zone of the city of Madrid and its province (750,000 inhabitants).
Each morning, RXR were obtained using a portable digital X-ray system. RXR were defined as X-rays obtained with this system on a programmed basis at the start of the daily work shift (8:00a.m.), with no clinical event or circumstance indicating the obtainment of X-rays. The study included patients over 15 years of age with serious trauma (Injury Severity Score (ISS)>15), admitted to the unit for 48h or more. Pregnant women were excluded, as were X-rays corresponding to the first 24h of admission, or indicated for specific reasons. Thus, we excluded X-rays indicated for clinical reasons or for performing invasive techniques or manipulating internal devices (central venous catheters, pulmonary artery catheters, orotracheal tubes, tracheostomy, thoracocentesis, endothoracic drains, gastrointestinal catheters, bronchoscopy, surgery, etc.).
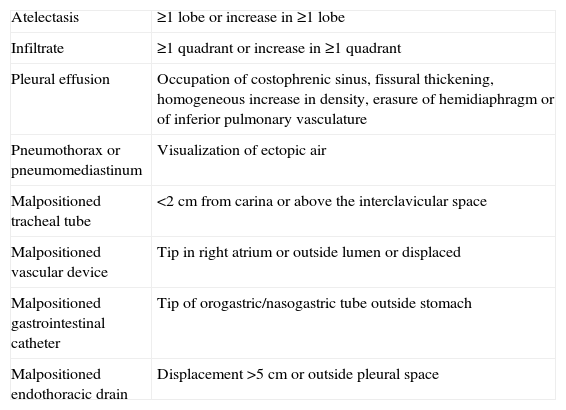
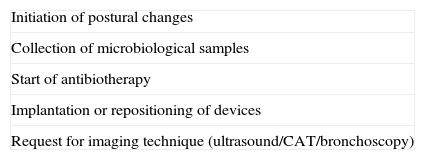
A strict definition was used for each study variable (new radiological findings, changes in clinical approach and in the clinical situation of the patient), as reflected in (Tables 1–3).4 The clinical–epidemiological data of the patients were collected (Table 4). A staff physician, freed from clinical tasks and not directly implicated in the study, checked the RXR obtained each day, in search of new radiological findings, according to the pre-established definitions. On the following day, the team in charge of patient care conducted a review to detect secondary changes in patient management in the hours after obtaining the X-ray. As predictive variables, changes were sought in the course of each patient during the day prior to obtainment of the X-ray–likewise according to pre-established definitions.
New radiological findings, appearance or significant increase of a phenomenon in the X-ray image.
| Atelectasis | ≥1 lobe or increase in ≥1 lobe |
| Infiltrate | ≥1 quadrant or increase in ≥1 quadrant |
| Pleural effusion | Occupation of costophrenic sinus, fissural thickening, homogeneous increase in density, erasure of hemidiaphragm or of inferior pulmonary vasculature |
| Pneumothorax or pneumomediastinum | Visualization of ectopic air |
| Malpositioned tracheal tube | <2cm from carina or above the interclavicular space |
| Malpositioned vascular device | Tip in right atrium or outside lumen or displaced |
| Malpositioned gastrointestinal catheter | Tip of orogastric/nasogastric tube outside stomach |
| Malpositioned endothoracic drain | Displacement >5cm or outside pleural space |
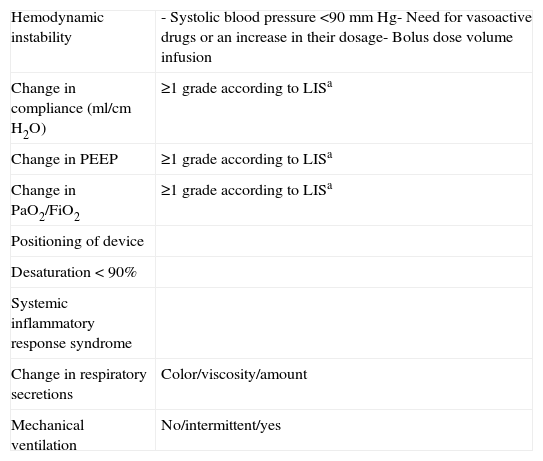
Changes in the clinical situation of the patient: events occurring in the 24h before the X-ray.
| Hemodynamic instability | - Systolic blood pressure <90mmHg- Need for vasoactive drugs or an increase in their dosage- Bolus dose volume infusion |
| Change in compliance (ml/cmH2O) | ≥1 grade according to LISa |
| Change in PEEP | ≥1 grade according to LISa |
| Change in PaO2/FiO2 | ≥1 grade according to LISa |
| Positioning of device | |
| Desaturation < 90% | |
| Systemic inflammatory response syndrome | |
| Change in respiratory secretions | Color/viscosity/amount |
| Mechanical ventilation | No/intermittent/yes |
The values of each variable were entered in a database (Access; Microsoft, Redmond, WA, USA) created to the effect.
Categorical variables are reported as relative frequencies (percentages), while quantitative variables are presented as the mean±standard deviation. The comparison of categorical variables was carried out using the chi-squared test, with a level of significance of p<0.05. The multivariate analysis involved a binary logistic regression model in which the dependent variable was the appearance of new findings in the RXR of the morning, and where the independent variables were included according to the statistical significance found in the univariate analysis and also the corresponding pertinence, normality and colinearity of the analyzed variables. The results of the multivariate analysis are expressed as the relative risk (RR) with the corresponding 95% confidence interval (95%CI).
The statistical analysis was carried out using the SPSS version 15 statistical package (SPSS Inc.; Chicago, IL, USA).
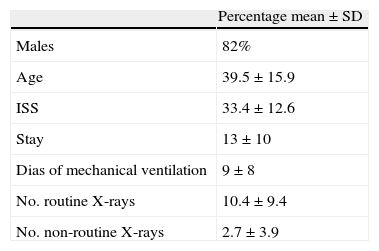
ResultsThe study covered a 12-month period between March 2006 and February 2007. At the end of this period the study was stopped, as sufficient significance was observed to reconsider our RXR prescription policy. We selected 138 patients and studied 1440 RXR (10.4±9.4 RXR/patient). The mean stay was 13±10 days. Most of the patients were males (81.9%). The distribution of the severity of chest trauma according to the Maximum Abbreviated Injury Score (MAIS) was: without injury (0) 45.3%, minor injury (1–2) 2.8%, and severe injury (3–5) 51.9%. The rest of the demographic and clinical–epidemiological variables are shown in (Tables 4 and 5).
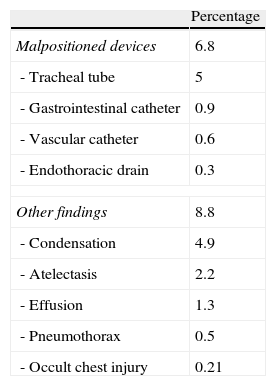
Eight RXR were lost to the effects of the analysis because of technical difficulties or traceability problems. Fourteen percent of the remaining RXR showed new findings (more than one in 1.5% of the cases). There were no new radiographic findings in 86% of the cases, while one finding was recorded in 12.5%, and two in 1.5% of the cases. The most frequent findings were the malpositioning of devices (6.8%) and lung infiltrates (4.9%). Table 6 reports the frequencies of the rest of the findings.
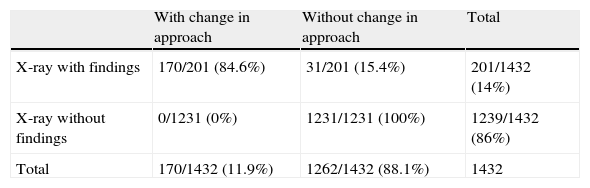
Relationship between the radiological findings and clinical changes.
| With change in approach | Without change in approach | Total | |
| X-ray with findings | 170/201 (84.6%) | 31/201 (15.4%) | 201/1432 (14%) |
| X-ray without findings | 0/1231 (0%) | 1231/1231 (100%) | 1239/1432 (86%) |
| Total | 170/1432 (11.9%) | 1262/1432 (88.1%) | 1432 |
We found 11.9% of the total RXR to induce a change in management approach; those with new findings accounted for 84.6% of these cases. Table 7 offers a more detailed account.
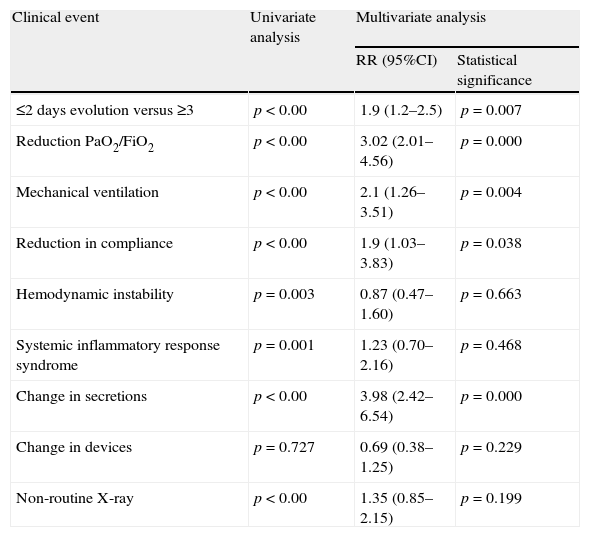
Univariate and multivariate analyses.
| Clinical event | Univariate analysis | Multivariate analysis | |
| RR (95%CI) | Statistical significance | ||
| ≤2 days evolution versus ≥3 | p<0.00 | 1.9 (1.2–2.5) | p=0.007 |
| Reduction PaO2/FiO2 | p<0.00 | 3.02 (2.01–4.56) | p=0.000 |
| Mechanical ventilation | p<0.00 | 2.1 (1.26–3.51) | p=0.004 |
| Reduction in compliance | p<0.00 | 1.9 (1.03–3.83) | p=0.038 |
| Hemodynamic instability | p=0.003 | 0.87 (0.47–1.60) | p=0.663 |
| Systemic inflammatory response syndrome | p=0.001 | 1.23 (0.70–2.16) | p=0.468 |
| Change in secretions | p<0.00 | 3.98 (2.42–6.54) | p=0.000 |
| Change in devices | p=0.727 | 0.69 (0.38–1.25) | p=0.229 |
| Non-routine X-ray | p<0.00 | 1.35 (0.85–2.15) | p=0.199 |
The analytical results were obtained by studying the relationship between the variables “clinical change the previous day” and “radiographic findings”, based on uni-multivariate and logistic regression analysis as described under Materials and methods section. The following predictors of new radiographic findings were identified: RXR corresponding to the first two days of admission, a decrease in PaO2/FiO2, Sat O2>90%, mechanical ventilation, a change in lung compliance, variation in the appearance of the respiratory secretions, and the obtainment of non-routine X-rays. The multivariate analysis identified the following significant predictive factors (p<0.05): RXR corresponding to the first two days of admission (RR 1.7; 95%CI 1.2–2.5), a decrease in PaO2/FiO2 (RR 3; 95%CI 2–4.5), mechanical ventilation (RR 2.1; 95%CI 1.2–3.5), a change in lung compliance (RR 1.9; 95%CI 1.1–3.5), and variation in the respiratory secretions (RR 3.9; 95%CI 2.4–6.5). The analytical results are reported in Table 7.
DiscussionTo our knowledge, this is the only study of its kind focused on traumatologic critical care patients. It has served to define the profile of the patient in which routine chest X-rays are most profitable in terms of changes in clinical management.
As limitations to the study, two fundamental points must be cited: the absence of X-ray evaluation by an independent radiologist, and the use of non-comparative methodology. Regarding the first point, in our setting it is not common to have a radiologist for daily evaluation of the RXR–this function being assumed by the clinician in charge of patient care. This fact may contribute to assimilate the study within the real-life application setting. In any case, we attempted to minimize bias through independent evaluation of the RXR by another clinician of the team. Regarding the lack of a comparative strategy, this has been the situation in most studies published to date. In any case, comparison efforts do not seem applicable with our current state of knowledge, due to few data available on the different strategies potentially open to comparison.
In our study, the number of RXR with new results was small (14%), though in contrast these findings proved useful in 84% of the cases. This might represent an argument both in favor and against the use of such X-rays. The solution could be a search for those situations which predict the appearance of radiological changes, making it possible to limit the X-ray requests to such situations, without losing performance or yield. In this sense, we observed a significant correlation with the prior presence of a decrease in PaO2/FiO2, the use of mechanical ventilation, a change in lung compliance, variations in the appearance of the respiratory secretions, and the obtainment of X-rays in the first two days of patient admission.
A similar approach was adopted by Fong et al.5 in 1995. Based on multivariate analysis in an inception cohort, these authors concluded that justification of RXR in the ICU is provided by the presence of a pulmonary arterial catheter. This study differed from our own in that it was carried out in a surgical ICU, and made use of definitions that do not coincide with our own. However, the proportion of findings (26%) and their yield (65%) proved similar.
The prospective studies conducted to date generally have considered the proportion of radiological results to be important (35% on average), though the proportions are lower than in the case of non-routine X-rays. In contrast, on examining their usefulness, most of them were of limited impact and did not lead to management changes. In the present study the yield reached only 14%, which falls well short of the 35% reported by most studies, but comes close to those recorded by the more recent studies such as that published by Graat et al.6 (6.6%), involving similar methodology and definitions. Our proportion of changes in management approach was 12%, which is intermediate between older studies (20%) and the work of Graat et al. (2.2%). On considering only the X-rays with findings, the proportion reaches 84%. In the remaining studies1–3,7–9 the estimate is 37%–Graat et al.6 reaching 32%, and Fong et al.5 65%. These discrepancies may be due to differences in the methods and definitions used, which moreover make comparisons difficult.
The low proportion of occult traumatic lesions first identified from RXR in this study may draw attention (0.21%). The anticipation of diagnoses through tertiary evaluations10 might explain such a low yield.
Most of the previous studies have been carried out in clinical, surgical or multidisciplinary ICUs. This would explain the fact that in our series (centered on trauma patients) males were more prevalent (82% versus 60%) and the mean age was younger (39 versus 65 years). The size of the sample and of the study Unit, the duration of follow-up, and the number of X-rays obtained were all intermediate in relation to the previous publications (3–28 beds, 80–754 patients, 220–2475 X-rays, and 4–25 months of follow-up).1,3,5,6,8,9,11,12
One of the main arguments against the policy of RXR refers to concern about radiation exposure of the patient and surroundings. In this sense, some studies3,13–15 show the cumulative environmental radiation to be below the risk level associated with the conventional protocols of use.
However, the strongest opposition to RXR refers to the resulting economical costs. In studies carried out during the 1990s, each X-ray implied a cost of about 75 USD (reaching 120 USD for the ultimate paying party). In relation to this issue, the existing studies are heterogeneous and difficult to compare, with sometimes even opposite results. Price et al.,16 in 1999, recorded important savings with the restrictive policy in a pediatric ICU in which 4550 RXR were obtained during 30 months. Other authors point to savings resulting from the anticipation of diagnoses. As an example, Brainsky et al.,8 in 1997, reported a saving of 98 USD per X-ray obtained. The current emphasis placed on cost savings and on the rationalization of resource utilization in healthcare, may ultimately limit the prescription of complementary tests to the conditions contemplated by closed protocols.17 The usefulness of control X-rays after the placement of internal devices has also been questioned. Possibly, instrumentations carried out in adequately monitored patients could be postponed or restricted to cases requiring increased precuations–with savings of up to 150 USD per X-ray.18–22
It is difficult to define a threshold of usefulness based on observational studies, regardless of the parameter chosen to the effect. In this context, comparative studies are needed, confronting the different strategies in reference to results of established relevance such as morbidity and mortality, stay or economical costs. Krivopal et al.,12 in 2003, compared the routine strategy with the restrictive protocol in a randomized prospective trial carried out in a clinical ICU with 20 beds. During 10 months the patients were assigned to the RXR group or to the group in which X-rays were obtained only upon specific indication. The latter group generated fewer X-rays, and there were no differences in the duration of mechanical ventilation, stay or mortality. This reduction in the number of X-rays was also associated to a reduction in costs and radiation exposure. Drawbacks to the study were its small sample size (94 patients), with none of the complex situations in which RXR could prove most useful (prolonged mechanical ventilation or ventilation in the prone position, transferred cases, etc.). It is therefore difficult to generalize the conclusions drawn.
Different authors analyzing the usefulness of RXR have found them to be scantly profitable,23,24 with no changes in patient morbidity or mortality after suppressing such X-rays. However, since these were not randomized studies, their results must be viewed with caution. Considering all the above, it might appear necessary to individualize the use of RXR. However, in the present situation this does not seem to be an acceptable and safe policy applicable to all settings–studies of greater quality being needed in order to draw firmer conclusions. Recently, Mets et al.,25 in a cardiothoracic unit, and Hendriske et al.,26 in a mixed clinical–surgical ICU, have helped clarify some ideas. After a change in radiological policy, involving the suppression of RXR, comparison of the two phases revealed good results in terms of mortality, stay and readmission rates after the change in strategy.
ConclusionThe risk of failing to identify hazardous conditions after suppressing routine X-ray practice seems to be low, and in contrast the decision may result in significant reduction in costs and radiation exposure. However, further studies are needed to confirm the results obtained in different types of patients.
Conflicts of InterestThe authors have no conflicts of interest to declare.
Please cite this article as: Chico Fernández M, et al. Predicción de la utilidad clínica de la radiografía de tórax rutinaria en una unidad de cuidados intensivos de traumatología. Med Intensiva. 2011;35:280–5.

